Venkat Arutla, MD1, Mark S. McFarland, MD, MSc2 1Rochester General Hospital, Rochester, NY; 2Rochester General Hospital, Pittsford, NY Introduction: It is common for patients to undergo cholecystectomy for gallbladder dysfunction, such as symptomatic cholelithiasis. This is usually a laparoscopic or open procedure that can sometimes result in complications. Some known complications of this surgery include bile duct injury and bile leak; however, these are relatively rare and have varying times of presentation. Here, we discuss a patient presenting with a late cholecystectomy complication.
Case Description/
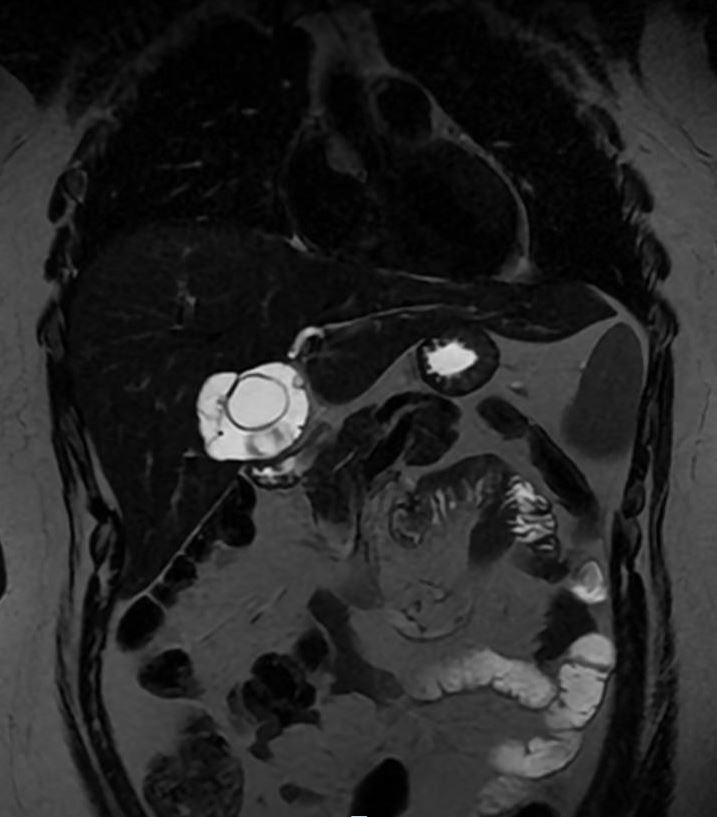
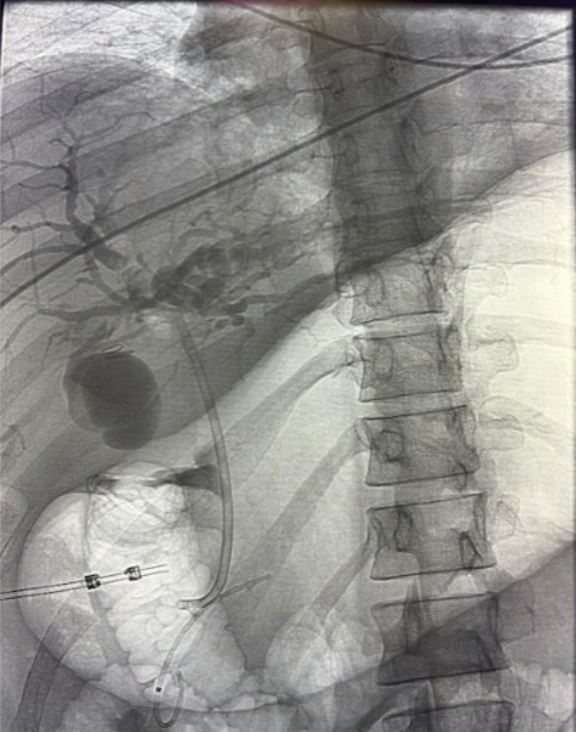
Methods: A 36 year old female with past medical history of polycystic ovarian syndrome, obesity and previous laparoscopic cholecystectomy converted to open 12 years ago, presented to the hospital with epigastric abdominal pain. Laboratory data revealed abnormal liver function tests with an elevated aspartate aminotransferase (AST) of 81, Alanine Aminotransferase (ALT) of 331 and total bilirubin of 3.7. She reported having similar symptoms earlier, along with dark urine and generalized pruritus. Computed tomography (CT) of the abdomen and pelvis and magnetic resonance cholangiopancreatography (MRCP) showed a 7.3cm multilobulated cystic lesion in the porta hepatis (Figure 1) concerning for a biloma causing extrinsic compression of the hepatic duct. The patient underwent endoscopic retrograde cholangiopancreatography (ERCP) with balloon occlusion cholangiogram under fluoroscopy. This showed contrast extravasation into the collection reported on previous imaging (Figure 2). Given external compression by the biloma, a stent was placed into the right common hepatic duct. The patient was later referred to surgery and underwent biloma drain placement with interventional radiology with plan for eventual surgical intervention. Discussion: Bilomas are known to occur 1-2 weeks post-operatively and usually present with abdominal pain, and sometimes with jaundice. This case is unique in that the patient was found to have a biloma 12 years after her cholecystectomy. The rarity of this presentation in a young patient may bias clinicians away from this diagnosis, even with knowledge of previous cholecystectomy. However, ERCP and surgical consultation could still be prudent in the management of a late-presenting biloma, especially in the context of extrinsic biliary compression.
Figure: Figure 1: MRCP revealing biloma.
Figure: Figure 2: ERCP showing contrast extravasation into biloma.
Disclosures: Venkat Arutla indicated no relevant financial relationships. Mark McFarland indicated no relevant financial relationships.
Venkat Arutla, MD1, Mark S. McFarland, MD, MSc2. P2258 - The Infamous Leak: A Late-Presenting Cholecystectomy Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.