Prerna Ashok Kherajani, MBBS1, Abdelkader Chaar, MD1, Abinash Subedi, MD1, Tessa Doolittle, MD2, Ola El-Zammar, MD1, Bishnu Sapkota, MD, FACG1 1SUNY Upstate Medical University, Syracuse, NY; 2SUNY Upstate Medical University Hospital, Syracuse, NY Introduction: Ectopic spleen auto-transplantation or splenosis is an uncommon and difficult to diagnose clinical entity that may occur following trauma or splenectomy. Usually, the splenic implants are located in the peritoneal cavity but occasionally can be in the chest or subcutaneous tissue; gastrointestinal tract involvement is rare. While the majority of the patients are asymptomatic, some develop complications like torsion, hemorrhage or rupture. Herein, we present an unusual case of ectopic spleen involving the stomach.
Case Description/
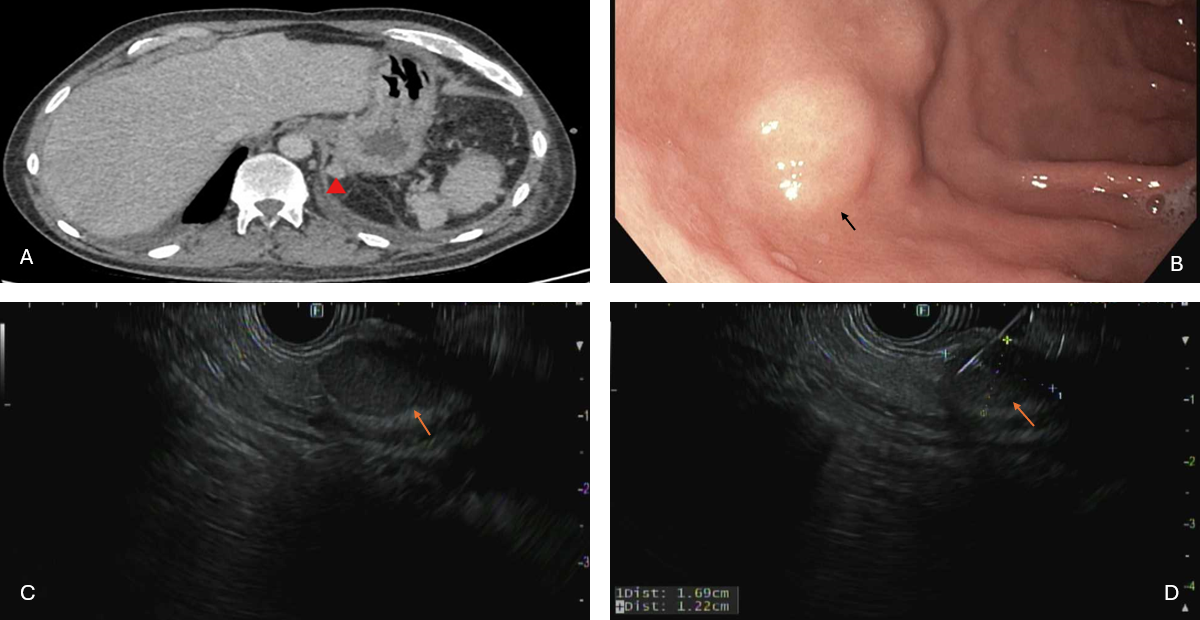
Methods: A 43-year-old male with a past medical history of right partial colectomy and partial splenectomy following a motor vehicle accident 20 years ago, recent exploratory laparotomy complicated by an enterocutaneous fistula was admitted for management of increased bilious output from the fistula and small bowel obstruction. Computerized tomography revealed an enhancing exophytic mass extending from the posterior gastric cardia (Figure 1A) for which gastroenterology was consulted due to concerns for a neoplasm. An endoscopic ultrasound showed a 17x8 mm oval hypoechoic lesion involving layers 4 and 5 with an exophytic component (Figures 1B-D). Fine needle aspiration revealed lymphoid aggregates and CD34 immunohistochemical stain showed splenic sinusoids supporting the diagnosis of ectopic spleen (Figure 2). As our patient was asymptomatic, monitoring was advised. Discussion: Most cases of splenosis are diagnosed incidentally on imaging or during surgeries performed for unrelated conditions. It poses a diagnostic challenge as it raises concerns for malignancy and can lead to extensive workup and procedures. The finding of splenic tissue within the gastric wall is particularly uncommon and reflects the migratory potential of splenic implants post-splenectomy. Diagnostic confirmation through imaging, such as technetium-99m-labeled heat-damaged red blood cell scans or biopsy, remains essential when splenosis is suspected. Endoscopic ultrasound remains an essential modality in evaluating similar lesions with gastrointestinal involvement. Our case raises awareness of this unusual diagnosis and highlights the importance of having a high index of suspicion in patients with relevant surgical or traumatic history.
Figure: A. Computed tomography abdomen/pelvis with contrast showed an enhancing exophytic mass extending from the posterior gastric cardia (red marker). B. Endoscopy revealed a single submucosal nodule with no bleeding and no stigmata of recent bleeding in the gastric fundus (black arrow). C, D. Endosonographically a 17x8 mm oval hypoechoic lesion involving layers 4 and 5 with an exophytic component was visualized (red arrows).
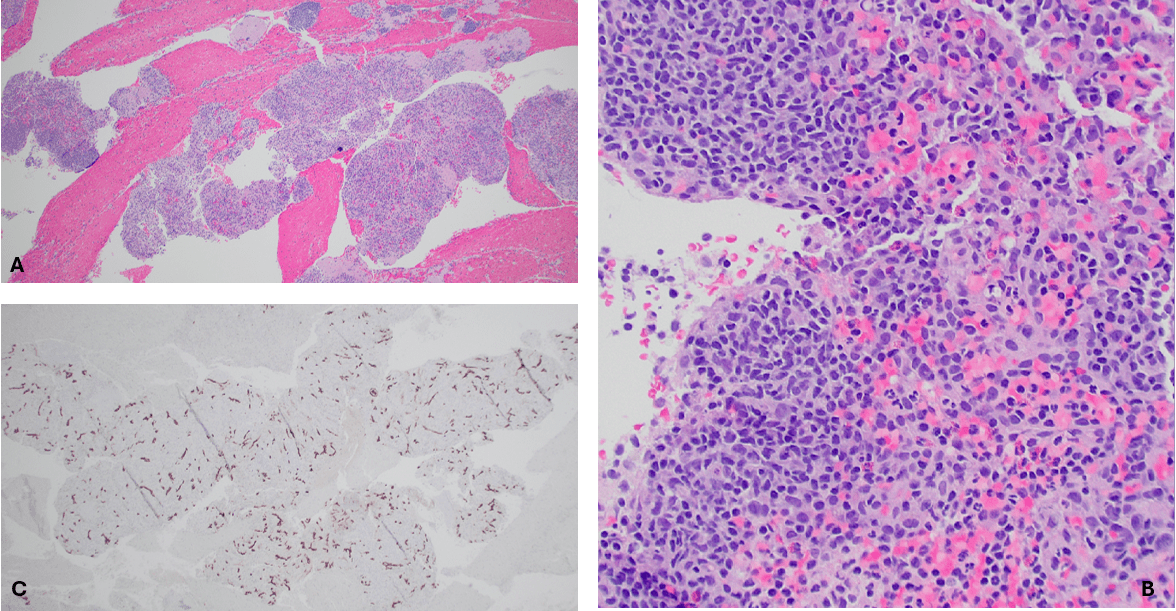
Figure: Fine needle aspiration surgical pathology: A. 4x magnification showing blood and splenic tissue. B. 20x magnification showing lymphoid aggregates. C. CD34 immunohistochemical stain showing splenic sinusoids.
Disclosures: Prerna Ashok Kherajani indicated no relevant financial relationships. Abdelkader Chaar indicated no relevant financial relationships. Abinash Subedi indicated no relevant financial relationships. Tessa Doolittle indicated no relevant financial relationships. Ola El-Zammar indicated no relevant financial relationships. Bishnu Sapkota indicated no relevant financial relationships.
Prerna Ashok Kherajani, MBBS1, Abdelkader Chaar, MD1, Abinash Subedi, MD1, Tessa Doolittle, MD2, Ola El-Zammar, MD1, Bishnu Sapkota, MD, FACG1. P2139 - Ectopic Splenic Tissue Masquerading as Gastric Tumor, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")