Felix Paredes-Gonzalez, MD, Patricia Rivera-Cariño, MD, Marilee Tiru-Vega, MD, Jaime Martinez-Souss, MD VA Caribbean Healthcare System, San Juan, Puerto Rico Introduction: Gastric cancer (GC) is one of the most common cancer related deaths worldwide. Signet ring carcinoma (SRC) is an indolent type of GC that accounts for 15-28% of the cases. It is usually found at advanced stages with poor prognosis on presentation. We present a case of a metastatic SRC presenting with esophageal dysphagia and ascites de novo.
Case Description/
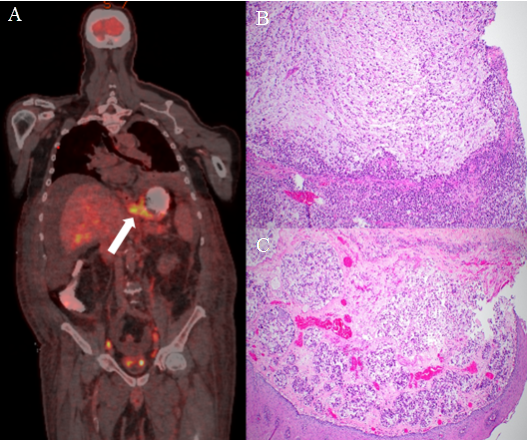
Methods: A 79-year-old man lifetime non-smoker, diagnosed with a saddle pulmonary embolism and deep venous thrombosis for 3 weeks, presents to the Emergency Department with increase abdominal girth, progressive esophageal dysphagia to solids and liquids and unintentional weight loss for 4 months. Physical exam revealed tension ascites. Laboratories showed neutrophilic leukocytosis and elevated alkaline phosphatase with normal transaminases. Three liters of ascitic fluid were removed and peritoneal fluid analysis was consistent with non-portal hypertension related etiology. Fluid cytology showed atypia of undetermined significance, been nondiagnostic for malignancy. A PET-CT scan revealed a hypermetabolic lesion at the gastroesophageal junction (GEJ), cardia and lesser curvature of the stomach (Figure 1A). Upper endoscopy from a year ago, exhibited a normal esophagus, mild antral granularity, normal cardia and fundal mucosa. Biopsies were negative for Helicobacter pylori. During hospitalization the patient complicated with sepsis and severe renal failure for which his family declined any invasive diagnostic procedures and opted for hospice care. Postmortem autopsy was consistent with a flat poorly defined mass involving the wall of the GEJ, fundus and antrum, that measured 9.0 x 8.0 cm. Histopathological examination of the stomach (Figure 1B) confirmed the diagnosis of poorly cohesive SRC with extensive metastatic spread to the esophagus (Figure 1C), lung, liver, pancreas and adrenals. Discussion: Clinicians should be aware of the aggressive nature of SRC, a subtype of diffused gastric cancer known for its submucosal spread which can lead to nonspecific symptoms, such as esophageal dysphagia, skin hyperpigmentation and ascites de novo in patients without preexisting liver disease. This, along with the potential to evade early endoscopic detection can be a real challenge to endoscopist. Physicians should maintain a high index of suspicion and careful endoscopic inspection is required.
Figure: Figure 1: PET-CT scan (A) showing a hypermetabolic lesion at the GEJ (white arrow); histopathology of the stomach (B) showing SRC; histopathology of the esophagus (C) consistent with metastatic spread of the SRC.
Disclosures: Felix Paredes-Gonzalez indicated no relevant financial relationships. Patricia Rivera-Cariño indicated no relevant financial relationships. Marilee Tiru-Vega indicated no relevant financial relationships. Jaime Martinez-Souss indicated no relevant financial relationships.
Felix Paredes-Gonzalez, MD, Patricia Rivera-Cariño, MD, Marilee Tiru-Vega, MD, Jaime Martinez-Souss, MD. P2118 - Peritoneal Whispers and Esophageal Alarms: Unmasking Gastric Signet Ring Cell Carcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.