Jiakai Pan, BA1, Hajra Jamil, MD2, Faisal Mehmood, MD3, Amar Thosani, MD4, Gavin Levinthal, MD5 1Midwestern University, Phoenix, AZ; 2Services Institute of Medical Sciences, Lahore, Pakistan, Glendale, AZ; 3HonorHealth, Glendale, AZ; 4HonorHealth, Scottsdale, AZ; 5Honor Health Gastroenterology - SCOTTSDALE, AZ, Scottsdale, AZ Introduction: Bouveret Syndrome is a rare form of gallstone disease causing gastric outlet obstruction. The terminal ileum is the most frequent impaction site in gallstone ileus, accounting for 60–70% of cases. It is more common in females, patients over 60, and those with a history of cholelithiasis. We present a case of a middle-aged man with gastric outlet obstruction caused by an impacted gallstone in the duodenal bulb.
Case Description/
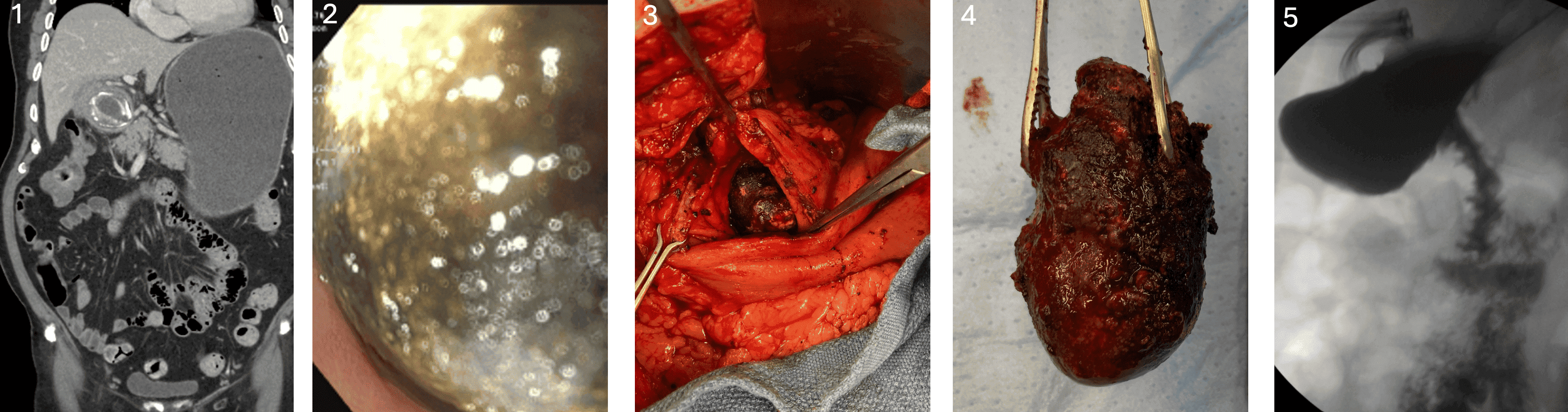
Methods: A 63-year-old man presented with a one-week history of worsening heartburn, abdominal pain, bloating, vomiting, and constipation. On examination, he was afebrile and hemodynamically stable. Laboratory studies revealed normal blood counts and renal function, but elevated liver enzymes, with AST at 144 U/L, ALT at 279 U/L, alkaline phosphatase at 94 U/L, and total bilirubin at 1.6 mg/dL. A computed tomography (CT) imaging revealed a distended stomach and a laminated, calcified lesion in the proximal duodenum consistent with a large gallstone eroding through the gallbladder wall into the duodenal bulb (Figure 1).
Esophagogastroduodenoscopy (EGD) showed retained gastric fluid, and a large gallstone impacted in the duodenal bulb (Figure 2). Electrohydraulic lithotripsy (EHL) was attempted but failed due to the stone’s hardness. The patient subsequently underwent exploratory laparotomy with gastrotomy, partial omentectomy, and successful removal of a 10 × 10 cm gallstone from the duodenal bulb (Figure 3 & 4). Postoperative upper GI series confirmed a cholecystoduodenal fistula (Figure 5). He recovered well and was discharged without complications. Discussion: Bouveret syndrome was first described in 1896 by French physician Léon Bouveret. Fewer than 320 cases have since been reported. Pathophysiology involves a gallstone entering the gastrointestinal tract via a fistula, often due to chronic cholecystitis. The cholecystoduodenal fistula is the most common type. Symptoms are nonspecific, including abdominal pain, nausea, vomiting, and bloating, making diagnosis challenging. CT imaging remains the gold standard. Endoscopy can aid in diagnosis and may allow for stone removal, but has a success rate under 10%. Surgery is often required. Whether to perform concurrent cholecystectomy and fistula repair remains debated, especially in elderly patients. In our case, due to age and absence of residual stones, simple stone extraction was deemed sufficient.
Figure: Figure 1). CT view of the distended stomach and a laminated, calcified stone eroding through the gallbladder wall into the duodenal bulb. Figure 2). EGD view of a large gallstone impacted in the duodenal bulb Figure 3 & 4). Exploratory laparotomy view of a 10 × 10 cm gallstone from the duodenal bulb and after extraction. Figure 5). Cholecystoduodenal fistula on UGI series
Disclosures: Jiakai Pan indicated no relevant financial relationships. Hajra Jamil indicated no relevant financial relationships. Faisal Mehmood indicated no relevant financial relationships. Amar Thosani indicated no relevant financial relationships. Gavin Levinthal indicated no relevant financial relationships.
Jiakai Pan, BA1, Hajra Jamil, MD2, Faisal Mehmood, MD3, Amar Thosani, MD4, Gavin Levinthal, MD5. P2105 - Bouveret’s Syndrome: A Classic Case of Gallstone Ileus Causing Complete Gastric Outlet Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.