University of Texas Health San Antonio San Antonio, TX
Grecia Dominguez Rivera, MD, Emilio Fernandez, MD, Juan Echavarria, MD University of Texas Health San Antonio, San Antonio, TX Introduction: Renal cell carcinoma (RCC) accounts for 3% of adult malignancies, resulting in over 13,000 deaths annually in the US, primarily due to metastases to organs such as the brain, liver, lungs, and bones. Metastases to the gastrointestinal tract are uncommon, with gastric involvement being particularly rare and typically presenting as polyps or ulcers that may mimic primary gastric carcinoma.
Case Description/
Methods: A 75-year-old male with a past medical history of aortic stenosis status post TAVR on dual antiplatelet therapy and RCC status post left radical nephrectomy (5 years before presentation) with lung metastasis, on immunotherapy, presented with a five-day history of melena. The heart rate at presentation was 70 bpm, and the blood pressure was 98/59 mmHg, with an otherwise normal physical examination. Labs showed a hemoglobin of 6.2 g/dL (baseline 15) and a BUN/Creatinine ratio of 42. An EGD was performed, revealing a non-bleeding cratered ulcer on the greater curvature of the gastric antrum. Biopsies were obtained, and the patient was discharged with recommendations to start PPI therapy while awaiting pathology results. Three days after the initial presentation, the patient was readmitted due to multiple episodes of large-volume hematemesis, with a repeat hemoglobin of 5.3 g/dL (from 8 at discharge). A repeat EGD showed the previously described ulcer with an adjacent area of active oozing, for which one clip was placed. The pathology report was consistent with metastatic RCC expressing AE 1/3, PAX8, and CA IX, after which the patient received radiation therapy without further bleeding episodes. A repeat EGD three months after diagnosis revealed punctate erythema and erosions in the body and antrum without definite ulceration. Biopsies were negative for malignancy. Discussion: Metastatic RCC to the stomach is rare, accounting for 0.2% to 0.7% of all RCC metastases. There is no distinct endoscopic pattern that reliably differentiates primary from secondary gastric tumors. This diagnostic challenge frequently leads to misclassification of these lesions as primary tumors or benign conditions (even in patients with a known primary malignancy), highlighting the need for histologic confirmation through biopsy. Given the rarity of gastric involvement, treatment requires a multidisciplinary approach that incorporates systemic therapy and local interventions (surgical resection, endoscopic removal, and radiotherapy).
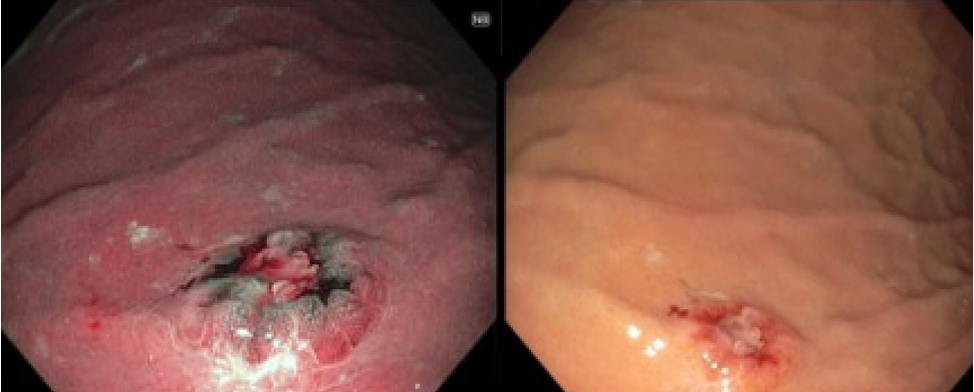
Figure: Non-bleeding cratered gastric ulcer on the greater curvature of the gastric antrum. The lesion was 6 mm in the largest dimension.
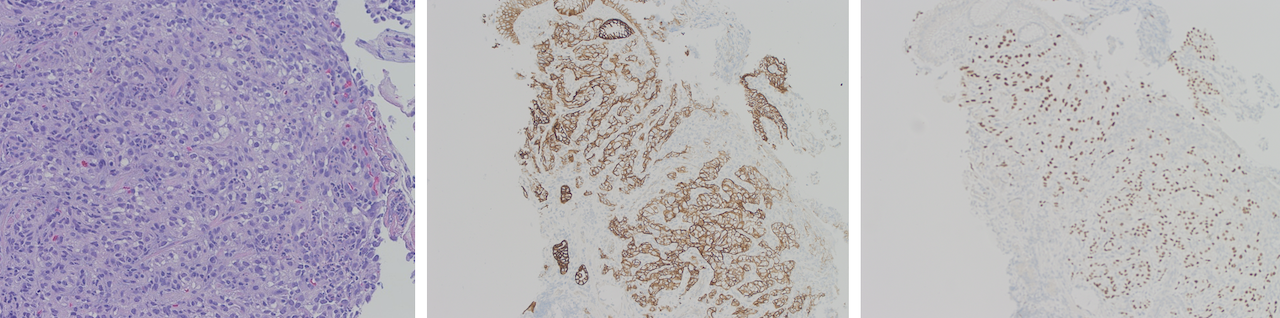
Figure: H&E stained section shows gastric mucosa with focal erosion associated with inflammation and a few admixed atypical cells showing clear cytoplasm and focally prominent nucleoli (Fig. 1). These atypical cells are positive for carbonic anhydrase IX (Fig. 2), and PAX8 (Fig. 3), supportive of involvement by metastatic clear cell renal cell carcinoma.
Disclosures: Grecia Dominguez Rivera indicated no relevant financial relationships. Emilio Fernandez indicated no relevant financial relationships. Juan Echavarria indicated no relevant financial relationships.
Grecia Dominguez Rivera, MD, Emilio Fernandez, MD, Juan Echavarria, MD. P2104 - When the Kidney Reaches the Stomach: A Rare Case of Gastric Metastasis from RCC, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.