MedStar Health-Georgetown/Washington Hospital Center Washington, DC
Qusai Al Zureikat, MD1, Marc El Khoury, MBBCh1, Sandeep Kowkuntla, BS2, Priyanka Kanth, MD3 1MedStar Health-Georgetown/Washington Hospital Center, Washington, DC; 2Georgetown University School of Medicine, Washington, DC; 3MedStar Georgetown University Hospital, Washington, DC Introduction: Breast cancer is the most common malignancy in women, but metastasis to the spleen is rare, and direct invasion into adjacent organs such as the stomach is even more unusual. This case highlights the importance of considering breast cancer in atypical presentations involving the spleen or gastrointestinal tract and highlights the critical role of immunohistochemistry in establishing the diagnosis.
Case Description/
Methods: A 66-year-old woman with a history of ER+/PR–/HER2+ invasive ductal carcinoma (IDC) of the breast, diagnosed in 2017, was treated with neoadjuvant TCHP, partial mastectomy, adjuvant trastuzumab, pertuzumab, radiation, and anastrozole. She had recurrence of her breast cancer in 2021 and was switched from anastrozole to exemestane. In April 2025, she presented with fevers, weight loss, and night sweats. Imaging revealed a large splenic mass with invasion into the gastric wall, along with an intramural gastric lesion. EGD showed a friable mass in the fundus and a 3 mm submucosal lesion on the greater curvature. Biopsies revealed poorly differentiated adenocarcinoma, positive for pancytokeratin, CK7, GATA3, and ER, and negative for CK20 and CDX2—findings consistent with metastatic breast carcinoma. The tumor was ER+/PR+/HER2–. Her condition deteriorated rapidly due to septic shock, renal failure, and worsening encephalopathy, ultimately leading to comfort care and death shortly after. Discussion: Splenic metastasis from breast cancer is exceedingly rare and often associated with widespread disease. Secondary invasion of the gastric wall from a splenic lesion is an unusual presentation that may mimic primary gastrointestinal malignancy. Immunohistochemical markers such as GATA3, CK7, and ER, combined with negative staining for CK20 and CDX2, are essential for confirming breast origin. Physicians should remain vigilant for atypical metastatic patterns in breast cancer survivors. Early recognition and multidisciplinary management are crucial, even when prognosis is poor.
Figure: Figure 1: EGD showing a friable mass in the gastric fundus
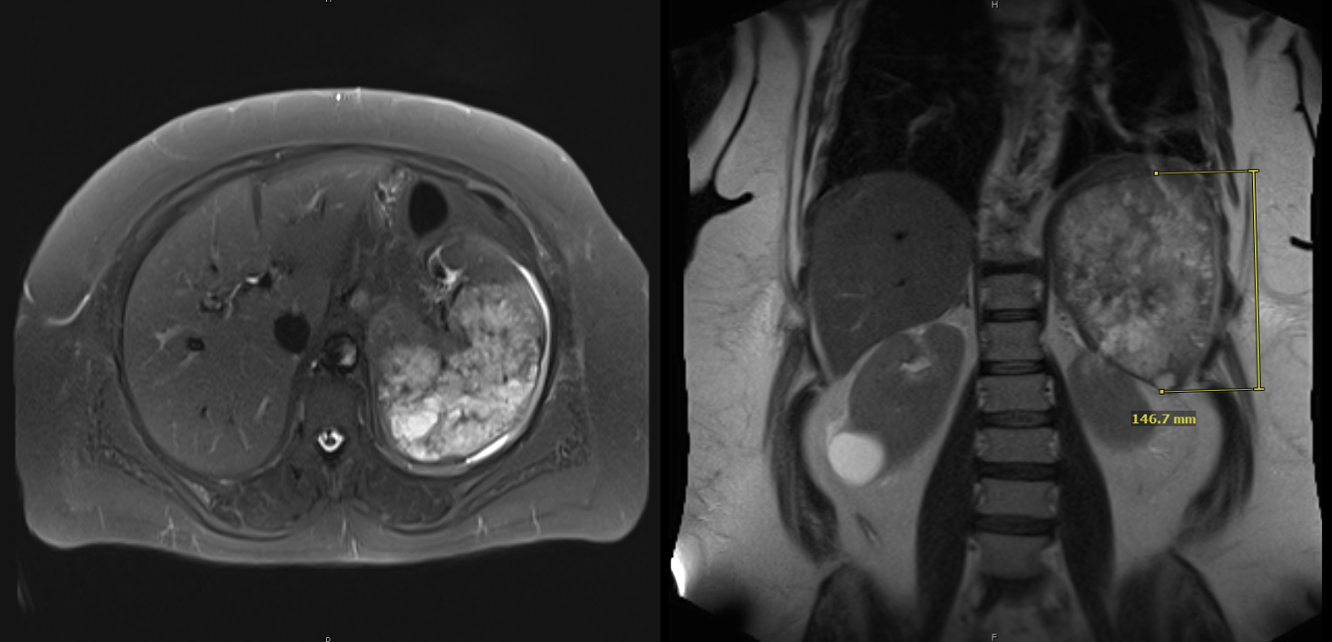
Figure: Figure 2: MRI showing a large splenic mass with invasion into the gastric wall
Disclosures: Qusai Al Zureikat indicated no relevant financial relationships. Marc El Khoury indicated no relevant financial relationships. Sandeep Kowkuntla indicated no relevant financial relationships. Priyanka Kanth indicated no relevant financial relationships.
Qusai Al Zureikat, MD1, Marc El Khoury, MBBCh1, Sandeep Kowkuntla, BS2, Priyanka Kanth, MD3. P2069 - Deceptive Lesions: Breast Carcinoma Presenting as a Splenic Metastasis With Gastric Wall Invasion, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")