King Faisal Specialist Hospital and Research Centre Ar Riyad, Ar Riyad, Saudi Arabia
Ali Kariri, MD, Muath Najmi, MD, Nawaf Bin Mugren, MD, Aymen Almuhaidb, MD, Badr Albawardy, MD King Faisal Specialist Hospital and Research Centre, Ar Riyad, Ar Riyad, Saudi Arabia Introduction: Immune checkpoint inhibitors (ICIs), such as pembrolizumab, are increasingly used in the treatment of malignancies but may cause immune-related adverse events (irAEs). While colitis is well recognized, gastritis is rare and can be misdiagnosed. We report a case of pembrolizumab-induced severe gastritis in a patient with uterine carcinoma.
Case Description/
Methods: A 55-year-old woman with stage IVB mismatch repair–deficient uterine endometrioid carcinoma received carboplatin, paclitaxel, and pembrolizumab, followed by maintenance pembrolizumab. Four months later, she developed intractable nausea, vomiting, and epigastric pain. She reported daily non-bloody emesis, anorexia, and a 4-kg weight loss over two weeks. CT imaging showed diffuse gastric wall thickening. Esophagogastroduodenoscopy (EGD) revealed erythematous, friable gastric mucosa with ulcerations. Histopathology showed chronic active gastritis with surface epithelial damage, glandular dropout, increased intraepithelial lymphocytes, and apoptotic bodies. Helicobacter pylori and viral inclusions were absent. Pembrolizumab was held, and she was started on oral corticosteroids and a proton pump inhibitor, resulting in significant clinical improvement. After two weeks, her symptoms markedly improved and she resumed oral intake. Repeat EGD after 10 weeks showed improvement in antral erythema, mucosal friability, and ulcerations. Biopsies demonstrated mild histologic improvement, though chronic active inflammation persisted. reinitiating of pembrolizumab was deferred due to ongoing mucosal activity. Discussion: ICI-induced gastritis is an under-recognized irAE involving T cell–mediated gastric injury. Diagnosis requires endoscopic and histologic confirmation with exclusion of other causes. Management depends on severity and may include corticosteroids. This case highlights the need for early recognition and treatment to minimize morbidity and allow for the possible reinitiating of immunotherapy.
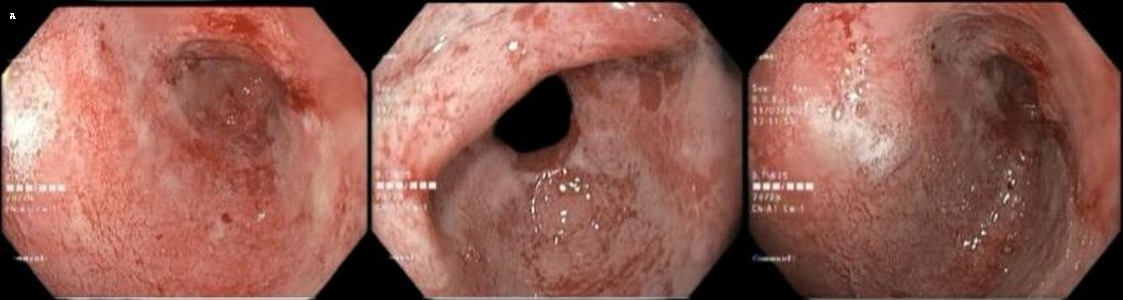
Figure: Figure A. Initial EGD images (A1–A3) showing diffuse erythema, mucosal friability, and ulcerations in the gastric body and antrum, consistent with immune checkpoint inhibitor-induced gastritis.
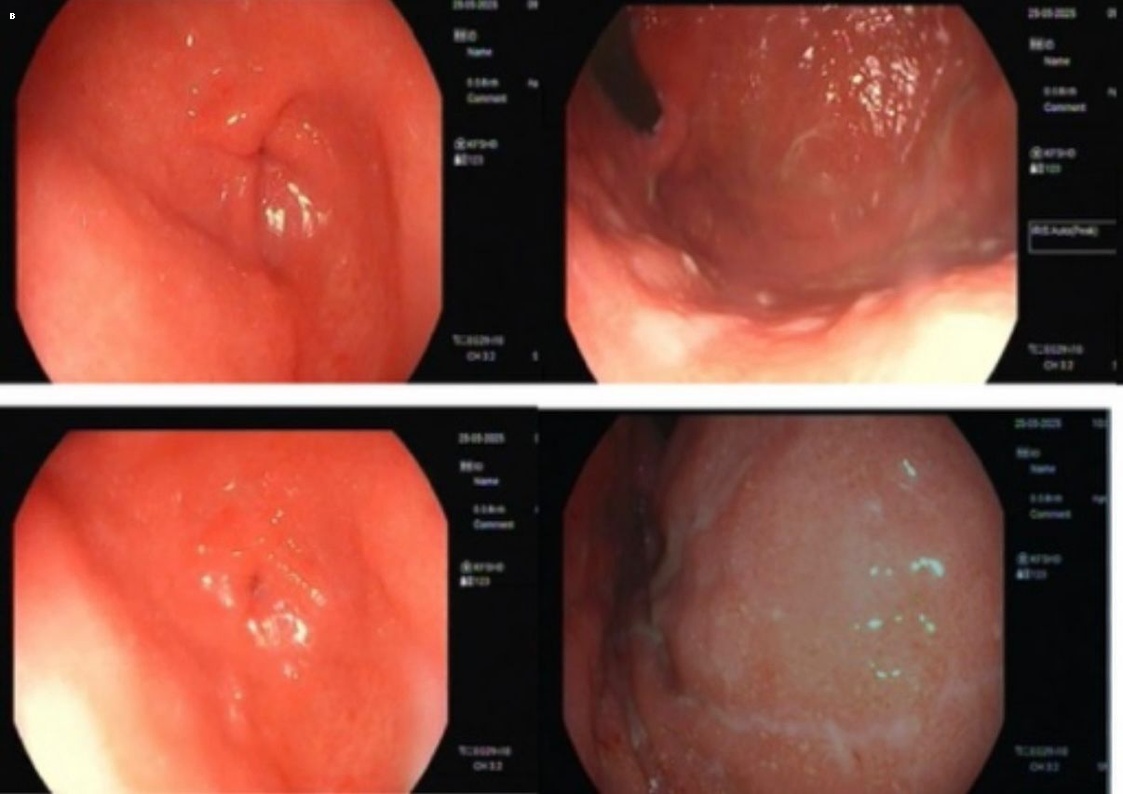
Figure: Figure B. Follow-up EGD after 10 weeks showing improved antral erythema, mucosal friability, and ulcerations in the antrum.
Disclosures: Ali Kariri indicated no relevant financial relationships. Muath Najmi indicated no relevant financial relationships. Nawaf Bin Mugren indicated no relevant financial relationships. Aymen Almuhaidb indicated no relevant financial relationships. Badr Albawardy indicated no relevant financial relationships.
Ali Kariri, MD, Muath Najmi, MD, Nawaf Bin Mugren, MD, Aymen Almuhaidb, MD, Badr Albawardy, MD. P2061 - When Immunotherapy Bites Back: Severe Gastritis From Pembrolizumab in a Uterine Carcinoma Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")