Sunday Poster Session
Category: Small Intestine
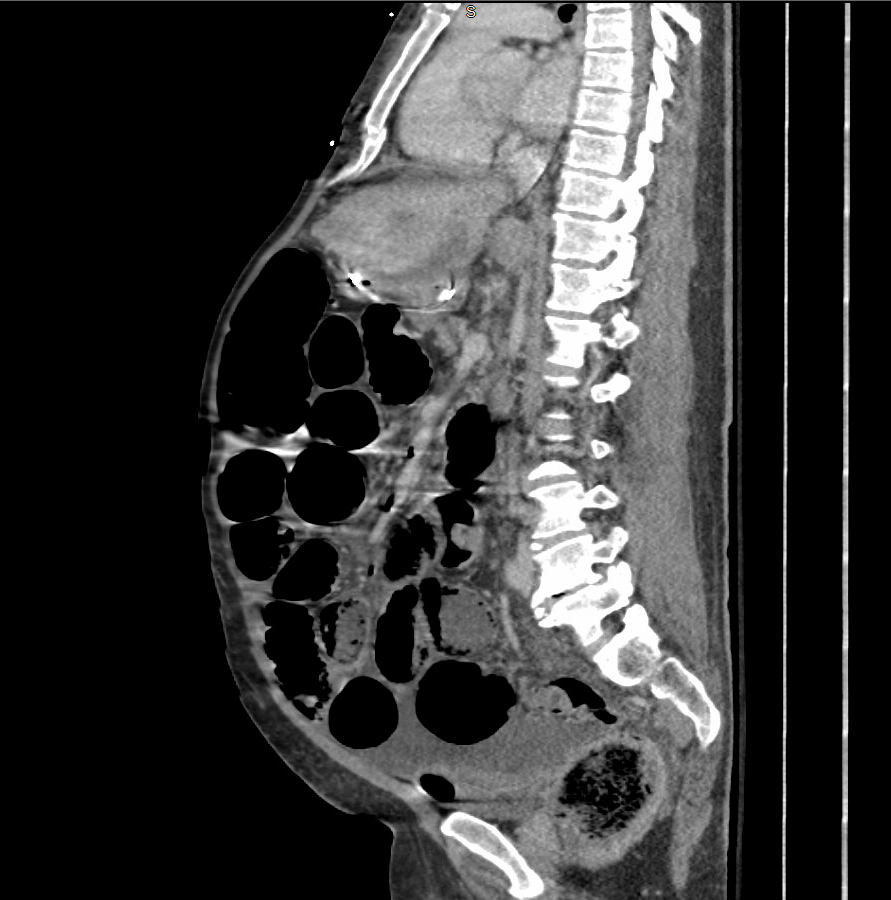
When Gas Crosses the Gut Wall: <i>Pneumatosis intestinalis</i> - Side Effect, Obstruction, or Ischemia?
 photo")
Balkrishna R. Sapariya, MBBS (he/him/his)
Western Reserve Health Education
Dayton, OH