Farah Issa, MD, Ameer Khalek, DO, Khalid Al Rayess, DO, Maklad Muthena, MD Dignity Health St Rose Dominican, Las Vegas, NV Introduction: The most common cause of extrahepatic bile duct injury is iatrogenic, typically observed following abdominal surgeries or endoscopic procedures involving cannulation of the biliary tract. Non-iatrogenic, traumatic bile duct injury is exceedingly rare, incidence 1–5 %. The vast majority of traumatic extrahepatic bile duct injury is secondary to penetrating trauma, blunt injury accounts for < 1 %. We present a case of distal common bile duct (CBD) injury following a motorcycle accident.
Case Description/
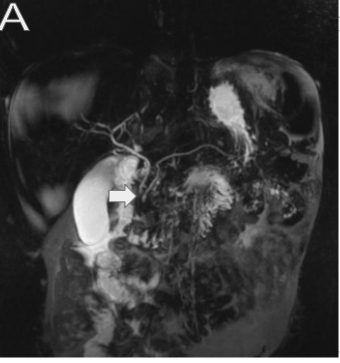
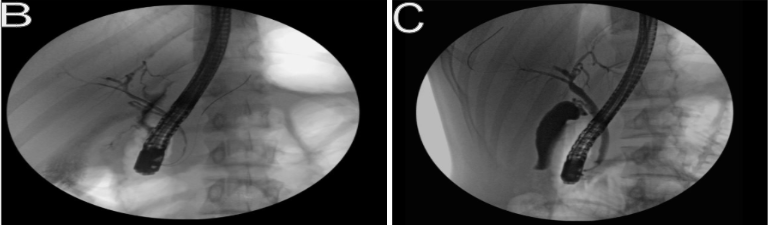
Methods: An 18-year-old male presents to the emergency department for evaluation following a motorcycle accident. The patient sustained blunt abdominal trauma after falling off his motorcycle. He presented with severe abdominal pain and nausea. Physical examination was notable for a diffusely tender abdomen. Initial labs notable for transaminitis- ALT 282 Unit/L, AST 280 Unit/L, Alkaline phosphatase 143 Unit/L, bilirubin 0.5 gm/dL. CT abdomen revealed grade V left hepatic lobe laceration, grade III right hepatic lobe laceration, and subcapsular liver hematoma. The patient was admitted to the ICU, he was managed conservatively and subsequently downgraded after an unremarkable course. On the fifth day of admission, bilirubin was noted to uptrend. The patient's physical exam remained unremarkable. Repeat imaging, abdominal CT revealed a new amount of free fluid in the peritoneum. Further imaging was pursued due to suspicion of bile leak. MRCP revealed caliber change at the distal CBD. HIDA scan revealed findings favoring a bile leak. ERCP was performed and confirmed a bile leak, contrast extravasation was noted in the distal CBD, near the ampulla. A 7 x 7 cm plastic stent was successfully deployed across the ampulla and past the bile leak. The stent was subsequently removed after 2 months, no further bile leak was noted. Discussion: Extrahepatic bile duct injury secondary to blunt trauma is relatively uncommon, and poses a diagnostic challenge. Delayed diagnosis is a frequent occurrence due to nonspecific symptoms and subtle presentation. Bile is relatively sterile, rendering peritoneal irritation minimal or absent. Clinicians should maintain a high index of suspicion for biliary trauma in the setting of blunt abdominal trauma. Uptrending bilirubin or jaundice should raise suspicion for biliary trauma, especially in the presence of concomitant visceral injury. Confirmation with imaging such as HIDA or MRCP is ideal. Most bile leaks resolve within 4-8 weeks with appropriate drainage.
Figure: Figure A: MRCP coronal view demonstrating caliber change of the distal CBD
Figure: Figure B &C: Pre and Post endoscopic retrograde cholangiopancreatography stent deployment
Disclosures: Farah Issa indicated no relevant financial relationships. Ameer Khalek indicated no relevant financial relationships. Khalid Al Rayess indicated no relevant financial relationships. Maklad Muthena indicated no relevant financial relationships.
Farah Issa, MD, Ameer Khalek, DO, Khalid Al Rayess, DO, Maklad Muthena, MD. P2357 - Beyond the Leak: Non-Iatrogenic Common Bile Duct Injury Secondary to Blunt Abdominal Trauma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.