
Monday Poster Session
Category: Colon
Vaibhav Rastogi, MD
Medical College of Georgia at Augusta University
Augusta, GA
Ogilvie’s syndrome or acute colonic pseudo-obstruction (ACPO) is characterized by marked colonic dilatation in the absence of a mechanical cause. Initial management typically includes supportive measures, neostigmine & colonoscopic decompression. In refractory cases, placement of a rectal tube for colonic decompression is often employed. However, tube dislodgement is a frequent limitation, compromising clinical efficacy. We describe a novel technique of endoscopic rectal tube fixation using endoclips at multiple colonic sites to enhance retention & therapeutic outcomes.
Case Description/
Methods:
An 80-year-old male was admitted to the ICU with acute metabolic encephalopathy, sepsis & ileus. Supportive management including correction of electrolytes, early ambulation & avoidance of opioids & anticholinergics had insufficient improvement. Pharmacologic intervention with 2 mg IV neostigmine produced minimal response. A decision was made to proceed with colonoscopic decompression & rectal tube placement.
A pediatric colonoscope was introduced via the rectum & carefully advanced to the cecum and decompressed first. The scope was withdrawn, and a Cook rectal tube with multiple side holes was selected, three thread loops were prepared; one at the tip, the 2nd approximately 12 inches proximal & the 3rd, 24 inches proximal from the tip. The colonoscope was reinserted while grasping the most distal loop with biopsy forceps. Upon reaching cecum, the loop was released, & two endoclips were deployed to anchor the loop to the cecal mucosa. The same technique was used to anchor the second loop to the transverse & the third loop to the descending colon. This provided fixation of the rectal tube at three key anatomical locations. The rectal tube was connected to a ureteric drainage bag. The tube remained in situ for four days, confirmed on imaging. The patient showed continuous clinical improvement. The tube eventually passed spontaneously per rectum on day 5.
Discussion:
Rectal tube dislodgement is a well-recognized challenge during management of ACPO. Our technique of securing the rectal tube with endoclips at the cecum, transverse & the descending colon provided enhanced stability & prolonged therapeutic decompression. This technique may minimize the risk of rectal tube dislodgement, reduce the need for repeated procedures or surgery & may serve as a valuable tool in the management of refractory ACPO. Larger cohort studies are needed to validate our approach.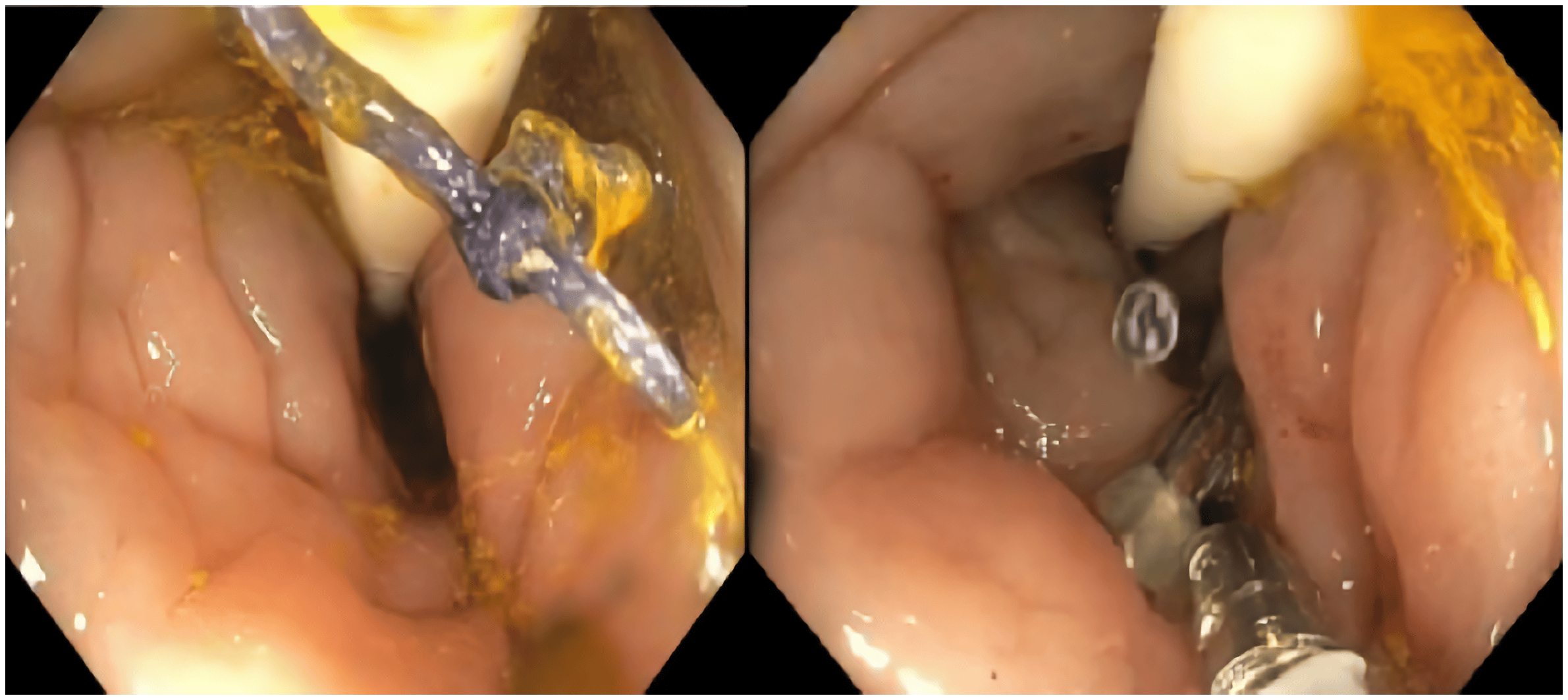
Figure: Figure 1: KUB showing improvement in colonic distention with rectal tube.
1A) Before procedure; 1B) Immediately after procedure; 1C) Day 3 after decompression tube placement; 1D) Day 5 showing near spontaneous passage of the tube.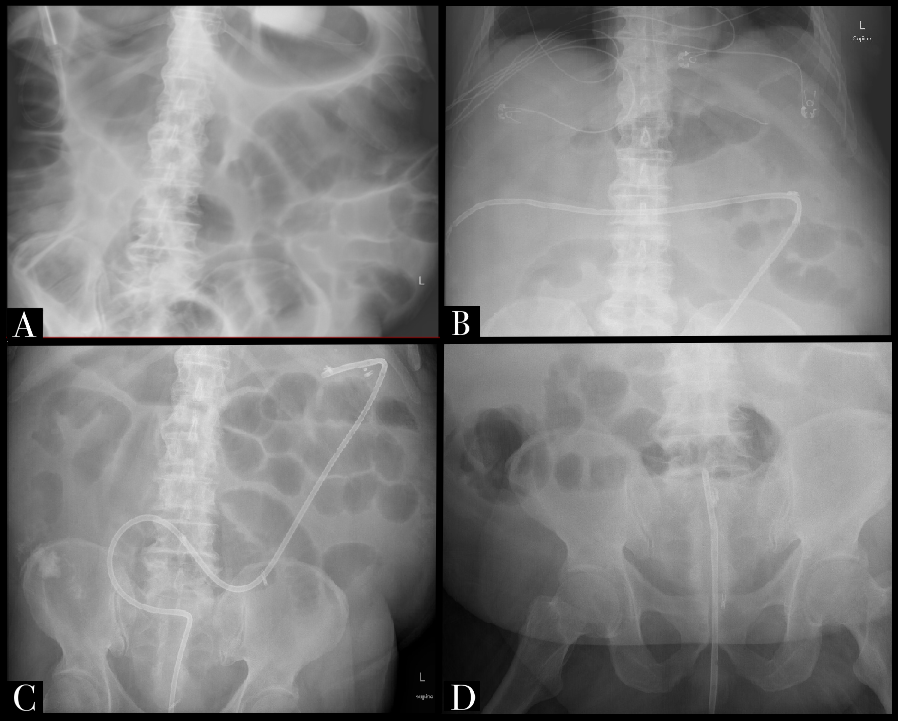
Figure: Figure 2: Colonoscopic rectal tube placement.
Disclosures:
Vaibhav Rastogi indicated no relevant financial relationships.
Raguraj Chandradevan indicated no relevant financial relationships.
Hrithik Dakssesh Putta Nagarajan indicated no relevant financial relationships.
Karansher Singh Randhawa indicated no relevant financial relationships.
Juliet Alderson indicated no relevant financial relationships.
Dowtin Mcknight indicated no relevant financial relationships.
Viveksandeep Thoguluva Chandrasekar indicated no relevant financial relationships.
Subbaramiah Sridhar indicated no relevant financial relationships.
Vaibhav Rastogi, MD1, Raguraj Chandradevan, MD2, Hrithik Dakssesh Putta Nagarajan, MBBS1, Karansher Singh Randhawa, MBBS1, Juliet Alderson, RN1, Dowtin Mcknight, RN1, Viveksandeep Thoguluva Chandrasekar, MBBS1, Subbaramiah Sridhar, MD2. P2548 - Anchoring Relief: Endoscopic Fixation of Rectal Tube for Bowel Decompression in Ogilvie’s Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.