Nikhita Kalra, MD1, Tanisha Kalra, MD2, Duaa Mohamed, MD1, Qi Yu, MD3 1SUNY Downstate Health Sciences University, Brooklyn, NY; 2SUNY Downstate Medical Center, New York, NY; 3SUNY Downstate, Brooklyn, NY Introduction: Ogilvie’s syndrome is characterized by colonic dilatation in the absence of an anatomic obstruction. It is mostly associated with constipation but can rarely present as secretory diarrhea. We present a case of the secretory diarrhea variant of Ogilvie’s syndrome causing severe refractory hypokalemia.
Case Description/
Methods: A 68-year-old male with asthma and chronic kidney disease presented with altered mental status and significant abdominal distension on exam. Labs showed acute respiratory acidosis which resolved with treatment. Imaging showed diffusely dilated bowel loops without a transition point. He developed severe persistent hypokalemia( < 2.5 mEq/L) refractory to aggressive repletion, further worsening the ileus. He then developed profuse watery diarrhea despite having constipation at baseline. Workup for diarrhea showed no infections, stool osmolality 304 mOsm/kg, stool potassium >100 mEq/L, and stool sodium < 20 mEq/L. The stool osmolar gap indicated secretory diarrhea. Stool and urine electrolytes revealed fecal potassium losses (elevated stool potassium and urine potassium-to-creatinine ratio of 10). He was diagnosed with the secretory variant of Ogilvie’s syndrome. Conservative management with nasogastric and rectal tube trials failed. Neostigmine was not used due to the risk of arrhythmias with severe hypokalemia. Endoscopic colonic decompression also failed. Treating the colonic dilatation was essential because the ongoing secretory diarrhea was contributing to severe hypokalemia. Promotility agents like prucalopride and erythromycin have been successful in isolated case reports but were declined by him due to their adverse effects. Spironolactone was initiated with subsequent dose adjustments to counteract aldosterone-mediated colonic potassium losses. Octreotide was initiated as a last resort given its effectiveness in some other cases of secretory diarrhea. He was discharged with a follow-up after hypokalemia resolved with spironolactone, octreotide, and daily potassium repletion. Discussion: The secretory diarrhea variant of Ogilvie’s syndrome is a rare disease. It can cause refractory hypokalemia due to the potassium losses from the overexpression of the Big Potassium (BK) channels in the colonic mucosa. Differentiation of urinary and fecal potassium losses is imperative. There are only a few case reports on this disease but no standard guidelines. This case seeks to help in the management of this disease through the use of aldosterone antagonists and somatostatin analogs.
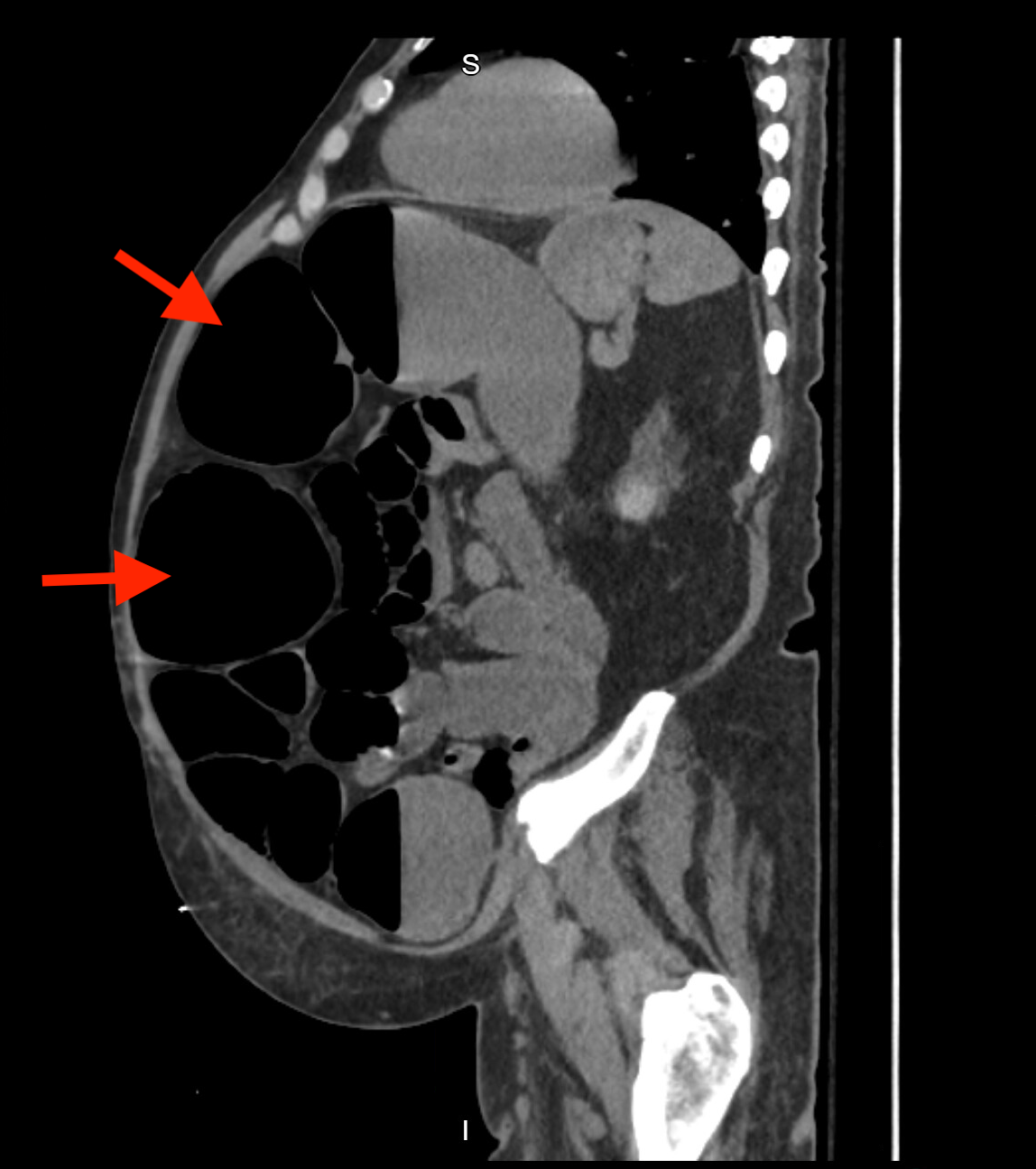
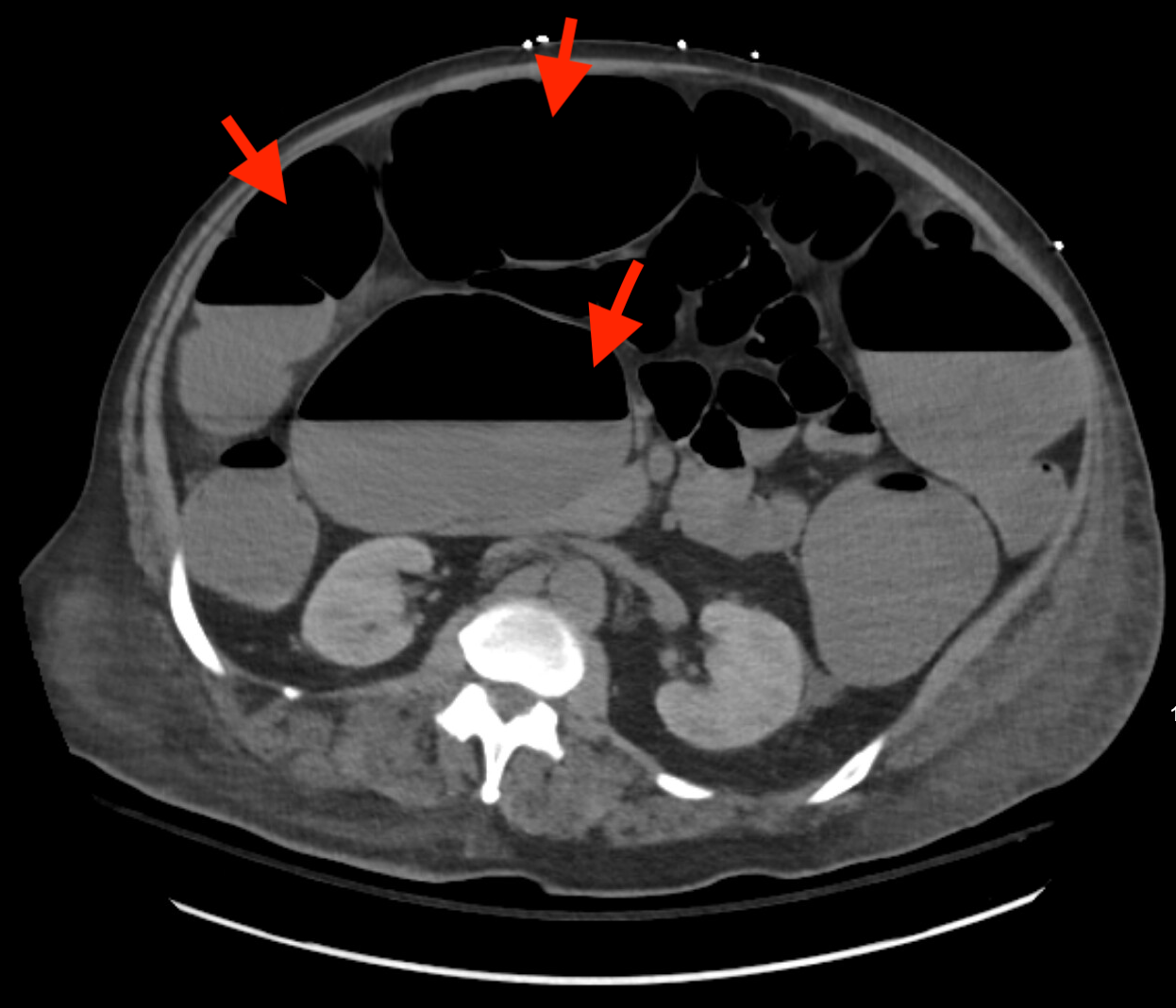
Figure: Computed tomography (CT) scan of the abdomen showing colonic dilatation without a transition point.
Figure: Computed tomography (CT) scan of the abdomen showing colonic dilatation without a transition point.
Disclosures: Nikhita Kalra indicated no relevant financial relationships. Tanisha Kalra indicated no relevant financial relationships. Duaa Mohamed indicated no relevant financial relationships. Qi Yu indicated no relevant financial relationships.
Nikhita Kalra, MD1, Tanisha Kalra, MD2, Duaa Mohamed, MD1, Qi Yu, MD3. P2601 - Uncharted Territory: The Secretory Diarrhea Variant of Ogilvie's Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")