
Monday Poster Session
Category: Endoscopy Video Forum
Mayank Goyal, MBBS
Mayo Clinic
Rochester, MN
Enterocutaneous fistula is an abnormal connection between intra-abdominal gastrointestinal tract and skin/wound resulting in drainage of intestinal contents through the abdominal wall. The majority of Enterocutaneous fistula occur in the post operative setting typically as a surgical complication like enterotomies and intestinal anastomotic dehiscence whereas spontaneous ECF, accounts for 20-30% is often associated with underlying pathologies such as Crohn's disease diverticulitis, radiation enteritis and malignancy. Patients with enterocutaneous fistula often experience a cascade of complications including sepsis, malnutrition, electrolyte imbalances and psychological distress significantly impacting patients' quality of life.
Case Description/
Methods:
We present a case of 77-year-old male patient with past medical history of cecal adenocarcinoma status post partial colon resection which was further complicated by fistula at the anastomotic site and treated with fistula plug and tissel glue. He remained asymptomatic for 8 years and recently presented with leakage from the same fistula site that on radiologic site suggested from the ileo colonic anastomosis
On CT we saw a fluid gas collection in the anterior abdominal wall with soft tissue thickening and matted small bowel which was representative of recurrent of possibly a new fistula or abscess.
On colonoscopy a 7mm fistula was noted at the previous anastomotic site. Firstly, the tract was threaded with guide wire, APC was loaded over the guidewire till start of the fistulous tract, wire was removed and we decided to de-epithelize the fistulous tract, by APC probe using argon plasma coagulation at 0.7 liters/minute and 70 watts in 1 cm increments, which was successful. Then, we used a 10x10 bilary fully covered self-expanding metal stent to stent this fistulous tract under fluoroscopic guidance. The stent was ultimately secured with two clips. The patient tolerated the procedure well and the post procedure fluoro showed absence of any leaks
Discussion:
We successfully demonstrate the management of enterocutaneous fistula using APC coagulation of the tract and biliary fully covered self-expanding metal stent.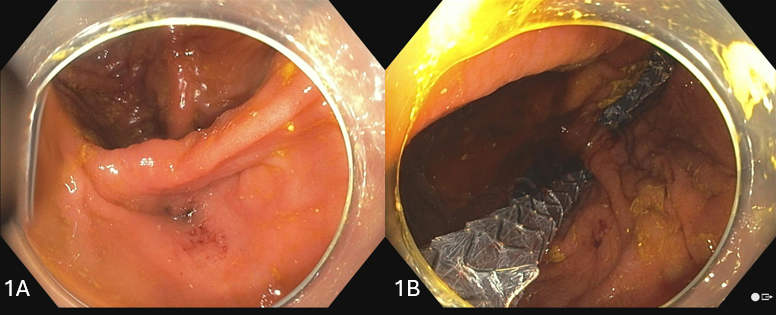
Figure: 1a- fistula
1b- fistula after stenting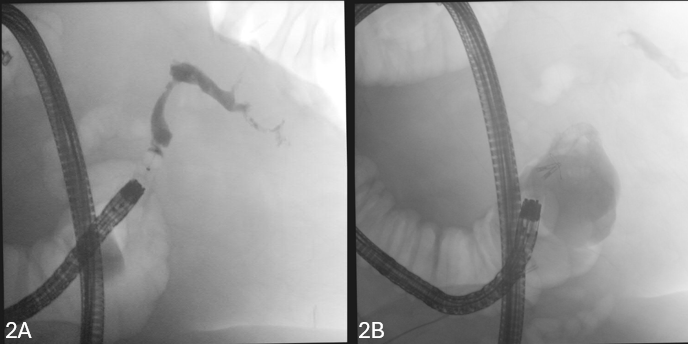
Figure: 2a- showing leak
2b- post procedure showing absence of leak
Disclosures:
Mayank Goyal indicated no relevant financial relationships.
Preeyati Chopra indicated no relevant financial relationships.
Ravneet Kaur indicated no relevant financial relationships.
Mahin Bhatt indicated no relevant financial relationships.
Ashwariya Ohri indicated no relevant financial relationships.
Khushboo Gala indicated no relevant financial relationships.
Navtej Buttar indicated no relevant financial relationships.
Mayank Goyal, MBBS1, Preeyati Chopra, MBBS2, Ravneet Kaur, MBBS1, Mahin Bhatt, MBBS1, Ashwariya Ohri, MBBS3, Khushboo Gala, MD1, Navtej Buttar, MD1. P2721 - Burn and Bridge: Enterocutaneous Fistula Closure With Argon Plasma Coagulation and Stenting, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.