Virginia Commonwealth University Health System Richmond, VA
Award: ACG Presidential Poster Award
Husam Mikati, MD1, Charles Leiner, MD2, Cathy Massoud, MD2, Christopher Gorman, MD2 1Virginia Commonwealth University Health System, Richmond, VA; 2Hunter Holmes McGuire VA Medical Center, Richmond, VA Introduction: A Gastroesophageal Reflux Disease (GERD) diet, which aims to reduce gastric acidity, can offer significant reflux symptom relief. However, if not applied judiciously, it may lead to unintended adverse effects. Scurvy, though, is not typically recognized as one of these potential complications can be a potential sequala. Scurvy, caused by vitamin C (ascorbic acid) deficiency, results in impaired collagen synthesis. Mucocutaneous findings of scurvy include diffuse perifollicular hemorrhages, corkscrew hairs, petechiae, ecchymoses, gingival hypertrophy, and bleeding. Other symptoms include arthralgias, swelling, ostealgia, fatigue, weakness, anemia, and delayed wound healing.
Case Description/
Methods: A 63-year-old man with GERD presented with four months of progressive left leg swelling, pain, and purpura. Despite wrapping the leg to alleviate the swelling, symptoms worsened. Examination of the left lower limb revealed purpura, xerosis, perifollicular hemorrhage, and corkscrew hairs on the shin, thigh, and buttocks (Figure 1). He had avoided citrus products and supplements for three years, managing GERD with a restrictive diet of chicken, rice, and peanut butter. Work-up for vascular, infectious, rheumatologic, and malignant causes was negative. The endoscopic evaluation did not suggest malabsorptive disease. An MRI of the left lower extremity showed marrow signal abnormalities consistent with bone marrow changes seen in scurvy. Skin biopsy was significant for perifollicular hemorrhages, corkscrew hairs, and mild perivascular inflammation, without vasculitis also indicative of changes that occur in scurvy (Figure 2). The clinical and histologic findings supported the diagnosis of scurvy. He started 500 mg of daily vitamin C, with symptom improvement at 3 months post-hospitalization. Discussion: Scurvy is typically linked to gastrointestinal risk factors like malabsorptive diseases, alcohol use disorder, and poor access to vitamin C-rich foods. However, this case highlights a rare cause: dietary restriction secondary to GERD. Scurvy doesn’t always follow classic generalized patterns; since collagen is widespread in the body, symptoms can vary. This patient had localized rather than generalized scurvy—without gingival symptoms or diffuse skin findings. MRI also showed bone marrow changes, a rarely noted sign of scurvy. Tight leg wrapping may have accelerated local symptoms. Clinicians should be aware that restrictive GERD diets may lead to scurvy and that its presentation can be atypical and focal.
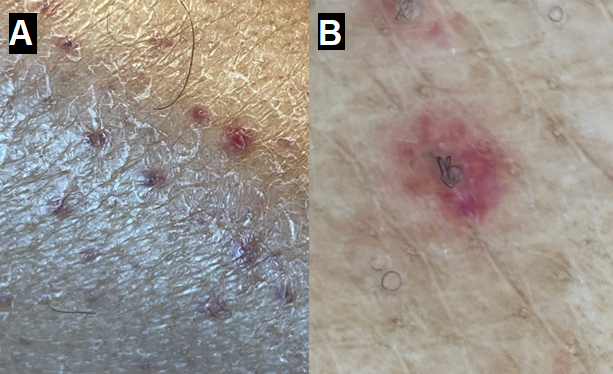
Figure: Figure 1: Clinical images of patient’s left lower extremity. (A) Scattered erythematous lesions on the anterior surface of the shin. (B) Corkscrew hairs with suspected perifollicular hemorrhage.
Figure: Figure 2: Photomicrograph of the punch biopsy from left lower extremity showing transected corkscrew hair (A) and dermal hemorrhage (B). These findings together are consistent with scurvy. Hematoxylin and eosin, original magnification x100.
Disclosures: Husam Mikati indicated no relevant financial relationships. Charles Leiner indicated no relevant financial relationships. Cathy Massoud indicated no relevant financial relationships. Christopher Gorman indicated no relevant financial relationships.
Husam Mikati, MD1, Charles Leiner, MD2, Cathy Massoud, MD2, Christopher Gorman, MD2. P2716 - An Unexpected Complication of a Self-Imposed Gastroesophageal Reflux Diet: Focal Scurvy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.