St. George's University School of Medicine Belmont, MA
Shreyas Kunjir, MD1, Vikash R. Chadive, MBBS2, Harman Sawhney, DO3, Taofeek Kolade, MD4, Philip Hall, MD, MPH4, Arsalan Ahmad, MD4, Karim Akl, MD5 1St. George's University School of Medicine, Belmont, MA; 2Bayonne Medical Center, North Bergen, NJ; 3CarePoint Health - Bayonne Medical Center, Melville, NY; 4CarePoint Health - Bayonne Medical Center, Bayonne, NJ; 5Jersey City Medical Center, Jersey City, NJ Introduction: Capsule endoscopy (CE) is a key modality in evaluating obscure gastrointestinal bleeding, offering direct visualization of the small bowel in a non-invasive manner. While generally safe, CE is not without risks. One of the most serious complications is capsule retention, which can lead to small bowel obstruction or, less commonly, perforation. Though rare—occurring in 2–8% of cases—retention poses a clinically significant threat that requires close monitoring, particularly in patients with potential small bowel pathology.
Case Description/
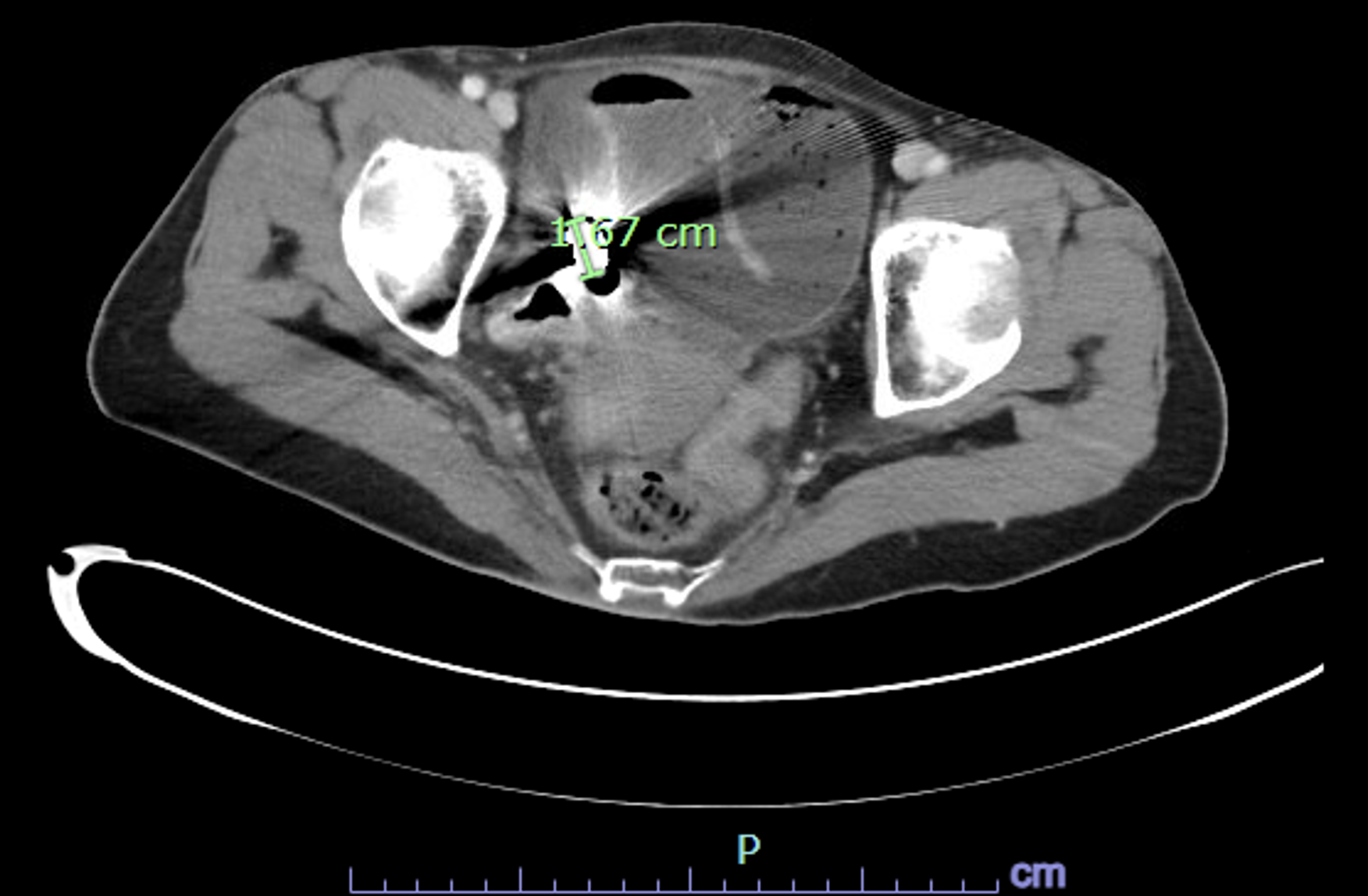
Methods: A 62-year-old woman with a history of recurrent GI bleeding underwent CE following unremarkable colonoscopy and an EGD that showed two non-bleeding gastric ulcers. Five days later, she presented with diffuse abdominal pain, bloating, nausea, and exertional shortness of breath. A CT scan showed capsule impaction in the right lower quadrant with proximal bowel dilation and free air, suggesting perforation (Figure 1).
Surgical consultation was obtained. At laparotomy, a 30 cm segment of ileum was resected. The capsule was freely mobile but just proximal to a strictured segment with creeping fat (Figure 2), raising concern for chronic inflammatory disease. Histology confirmed a fibrotic stricture. The patient had an uncomplicated recovery and was discharged home four days postoperatively (Figure 2). Discussion: While CE is widely used and generally well tolerated, capsule retention remains a known complication, especially in those with unrecognized strictures. Retention is defined as the capsule remaining in the GI tract for over two weeks or requiring removal due to symptoms. Common causes include Crohn’s disease, NSAID enteropathy, tumors, or prior radiation. This patient had no known IBD, though intraoperative findings suggested subclinical Crohn’s.
Symptoms of retention may be delayed, with obstruction appearing days to weeks later. Any patient with new abdominal symptoms after CE should undergo prompt imaging. In this case, early recognition and surgical intervention prevented greater morbidity. Pre-procedural screening—via cross-sectional imaging or a patency capsule—can help identify high-risk patients. Patients should also be counseled about this complication.
This case underscores the need for caution when using CE in patients with possible small bowel disease and highlights the importance of post-procedural monitoring. Though rare, capsule retention can become a surgical emergency if not quickly addressed.
Figure: Figure 1 Computed tomography (CT) showing the capsule endoscope impacted in the ileum (green label, 1.67cm.) with small bowel dilation along with free peritoneal air.
Figure: Figure 2 Surgical specimen of resected small bowel segment containing the capsule (marked by surgeon’s finger). Removed capsule endoscope in subsequent image.
Disclosures: Shreyas Kunjir indicated no relevant financial relationships. Vikash Chadive indicated no relevant financial relationships. Harman Sawhney indicated no relevant financial relationships. Taofeek Kolade indicated no relevant financial relationships. Philip Hall indicated no relevant financial relationships. Arsalan Ahmad indicated no relevant financial relationships. Karim Akl indicated no relevant financial relationships.
Shreyas Kunjir, MD1, Vikash R. Chadive, MBBS2, Harman Sawhney, DO3, Taofeek Kolade, MD4, Philip Hall, MD, MPH4, Arsalan Ahmad, MD4, Karim Akl, MD5. P3033 - Swallowed but Not Forgotten: A Capsule’s Journey to Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")