Nina Devas, MD1, Firrah Saeed, MD1, Carolyn Wilson, MD2, Alyssar Habib, MD1, Cyrena Lam, MD3, Violeta Popov, MD, PhD2 1NYU Grossman School of Medicine, New York, NY; 2NYU Langone Health, New York, NY; 3NYU Langone Health, New York City, NY Introduction: Appendiceal mucoceles are rare, often asymptomatic lesions typically discovered incidentally during imaging or endoscopy. They may mimic other pathologies, such as intussusception or appendicitis, and have potential for malignant transformation, making early detection and appropriate management critical. We present a case of an incidental appendiceal lesion found during routine colonoscopy in an asymptomatic patient, ultimately found to be a benign process.
Case Description/
Methods: A 57-year-old male with hypertension, hyperlipidemia, and paroxysmal atrial fibrillation, presented for his first screening colonoscopy. He had no family history of colorectal cancer. He denied any gastrointestinal symptoms including abdominal pain, changes in bowel habits, hematochezia, melena, weight loss, or anorexia. Physical examination and vital signs were unremarkable, with no abdominal tenderness, distension, or palpable masses. There were no abnormal lab values on comprehensive metabolic panel or complete blood count.
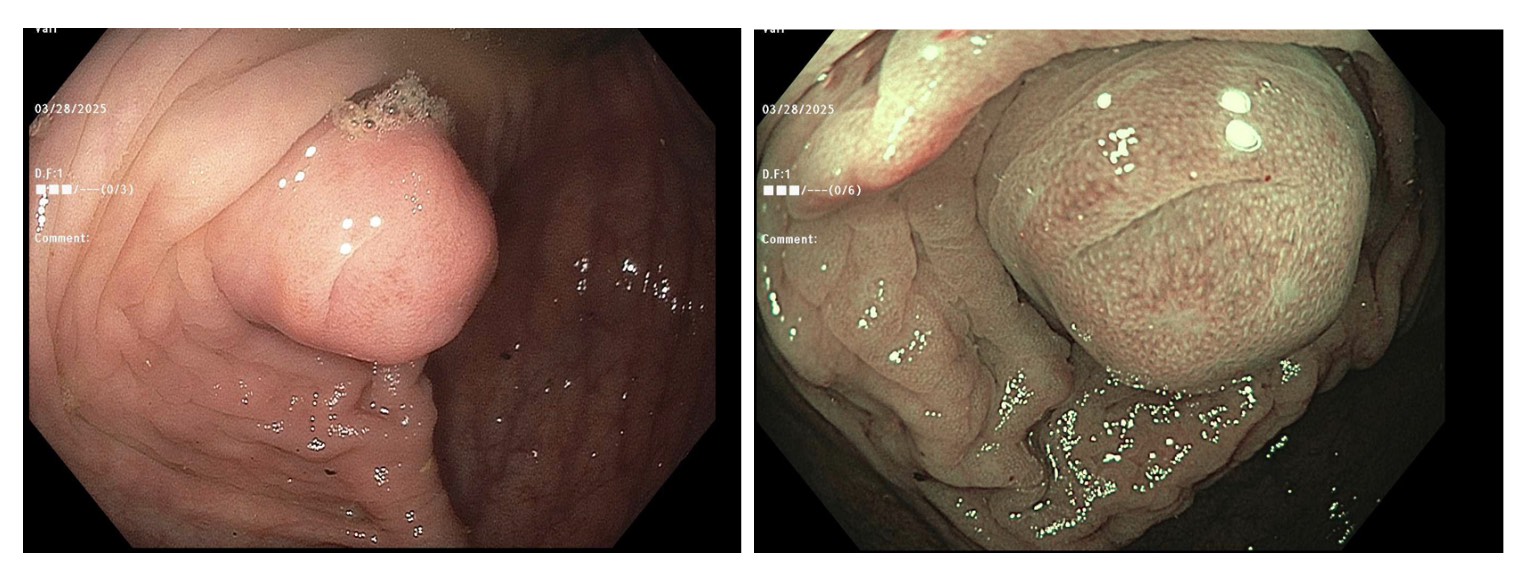
Colonoscopy revealed a prominence at the appendiceal orifice, suggestive of either intussusception of the appendix or a mucocele. The patient was then sent for CT abdomen and pelvis, which showed a proximal appendiceal dilation (18x13mm) without contrast filling, periappendiceal fatty infiltration, appendicolith, or intraluminal gas. This was suspicious for mucocele, although early appendicitis can present radiographically similar. The patient was referred to general surgery for further evaluation.
Biopsies taken from the appendiceal orifice showed polypoid colonic mucosa with a lymphoid aggregate, without evidence of dysplasia. Despite benign biopsy findings, a laparoscopic cecectomy is planned for definitive diagnosis and treatment. Discussion: Appendiceal mucoceles have an estimated incidence of 0.2–0.7% of appendectomy specimens. They are divided histologically into four subtypes: benign retention cyst, mucous hyperplasia, mucinous cystadenoma with low-level dysplasia, and mucinous cystadenocarcinoma. Most are found incidentally, as in this case. Colonoscopy may reveal a bulge or prominence at the appendiceal orifice, but diagnosis typically requires imaging and histology. Given the risks of misdiagnosis, surgical resection is recommended to confirm pathology and prevent complications. This case highlights the importance of recognizing appendiceal abnormalities during routine colonoscopy and emphasizes the role of imaging and surgical evaluation in managing such incidental findings.

 photo")