Harleen Chela, MBBS, MD1, Nisar Amin, MD2, Omer Elfeky, MD2, Ebubekir Daglilar, MD2, Veysel Tahan, MD, FACG3 1West Virginia University Charleston Area Medical Center, South Charleston, WV; 2Charleston Area Medical Center, Charleston, WV; 3Northeast Ohio Medical University & CAMC, Charleston, WV Introduction: Acute gastrointestinal bleeding secondary to peptic ulcer disease is a relatively common cause of hospitalization and can sometimes require measures beyond endoscopy to achieve hemostasis. Interventional Radiology is often able to perform embolization of an actively extravasating blood vessel especially when the gastrointestinal bleed is refractory to endoscopic measures. We present a case of an unusual finding on upper endoscopy showing exposed coils in the base of the duodenal ulcer.
Case Description/
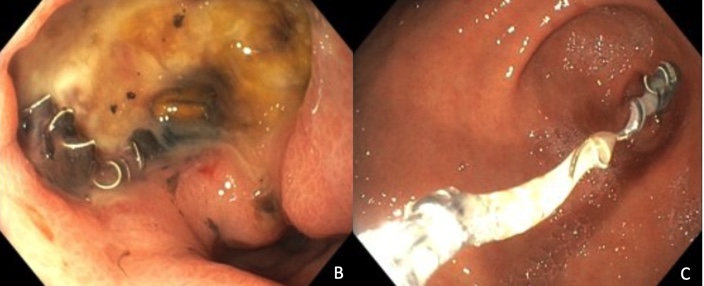
Methods: A 66-year-old male with past medical history significant for chronic alcohol use, prior history of gastric ulcers presented with acute onset of hematochezia. He was found to be in hemorrhagic shock and was aggressively resuscitated. On examination, was tachycardic, hypotensive and tender on palpation of upper abdomen. Hemoglobin on presentation was 3.8 gm/dl with no prior baseline for comparison. Platelet count was normal the INR was elevated at 2.21. CTA of the abdomen showed postembolization coiling of the gastroduodenal artery (GDA) with adjacent duodenitis and possible peptic ulcer disease involving the proximal duodenum (Figure A). No active extravasation who was found. Upper endoscopy was performed and showed a large duodenal bulb ulcer measuring about 2.5 cm nose clean based. However there was note of 2 coils that were seen in the ulcer base with one that had almost completely eroded through the ulcer and appeared to be no longer attached so it was gently removed using cold biopsy forceps (Figures B, C). Further attempts were not made to remove the second coil. Interventional Radiology was consulted and angiography of the celiac and superior mesenteric arteries demonstrated no flow to the GDA from the celiac artery. However retrograde filling of the GDA via the superior mesenteric, through inferior pancreaticoduodenal artery (IPDA) was seen. Embolization of the IPDA and GDA was performed. After this no further GI bleeding was noted, however patient had complicated hospital stay and eventually succumbed to respiratory failure. Discussion: Refractory peptic ulcer disease that is not responsive to endoscopic measures after and requires Interventional Radiology assistance with angiography and embolization. Embolization of the gastroduodenal artery is a commonly performed procedure, especially for peptic ulcers arising in the duodenal bulb. It is uncommon for embolization coils to be visible in the ulcer base and even more so for them to be removed without precipitating bleeding.
Figure: Figure A: CTA of the abdomen showed postembolization coiling of the gastroduodenal artery.
Figure: Figures B,C: Large duodenal ulcer with emboilzation coils seen in the base and one of them being gently removed.
Disclosures: Harleen Chela indicated no relevant financial relationships. Nisar Amin indicated no relevant financial relationships. Omer Elfeky indicated no relevant financial relationships. Ebubekir Daglilar indicated no relevant financial relationships. Veysel Tahan indicated no relevant financial relationships.
Harleen Chela, MBBS, MD1, Nisar Amin, MD2, Omer Elfeky, MD2, Ebubekir Daglilar, MD2, Veysel Tahan, MD, FACG3. P3025 - Exposed Embolization Coils: An Unusual Finding on Upper Endoscopy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.