Aishwarya Gatiganti, MD1, Husayn F. Ramji, MD2, John M. Bloch, MD1 1Tulane School of Medicine, New Orleans, LA; 2Tulane University School of Medicine, New Orleans, LA Introduction: Mantle Cell Lymphoma (MCL) is a subtype of non-Hodgkin lymphoma associated with the t(11;14)(q13;q32) chromosomal translocation and has a wide range of presentations ranging from indolent non-nodal disease to aggressive blastoid type. It most commonly presents in the lymph nodes, but can have extra-nodal presentations in the spleen, bone marrow, and gastrointestinal (GI) tract. GI tract involvement is usually restricted to the stomach and colon, but less commonly involves the duodenum and rectum. Although found histologically, only 30% of MCL are associated with gross changes on endoscopy. This case discusses a patient with advanced stage MCL who presented with a chief complaint of hematochezia, ultimately found to have significant duodenum and rectal mucosal involvement secondary to MCL.
Case Description/
Methods: An 84-year old male with pertinent past medical history of stage III mantle cell lymphoma t(11;14) diagnosed five months prior presented to the emergency department with a one day history of altered mental status (AMS) and hematochezia after recent initiation of apixaban for a deep vein thrombosis. The patient was admitted for further workup and management, with labs significant for a urinary tract infection and hemoglobin of 9.1. While inpatient, imaging revealed mediastinal, mesenteric, and inguinal adenopathy, as well as diffuse rectal wall thickening, concerning malignancy versus proctitis. Gastroenterology was consulted and proceeded with upper and lower endoscopy. Both upper and lower GI endoscopy revealed diffuse nodular changes as well innumerable sessile polyps in the duodenum, as well as a severely nodular and edematous rectal mucosa. Biopsies of both the duodenum and rectum demonstrated mantle cell lymphoma. After goals of care discussion with patient and family, the decision was made to proceed with hospice care instead of further treatment. The patient ultimately passed away in hospice care two months after this admission. Discussion: Here we present a common cause for hospitalization, hematochezia, with an unusual etiology of advanced MCL with extensive duodenal and rectal mucosal involvement. This case emphasizes the importance of keeping a broad differential when it comes to lower GI bleeds, particularly when considering endoscopic management as mucosal bleeding such as this is less likely to be amenable to standard endoscopic hemostasis techniques of hemostatic clips and electrocautery.
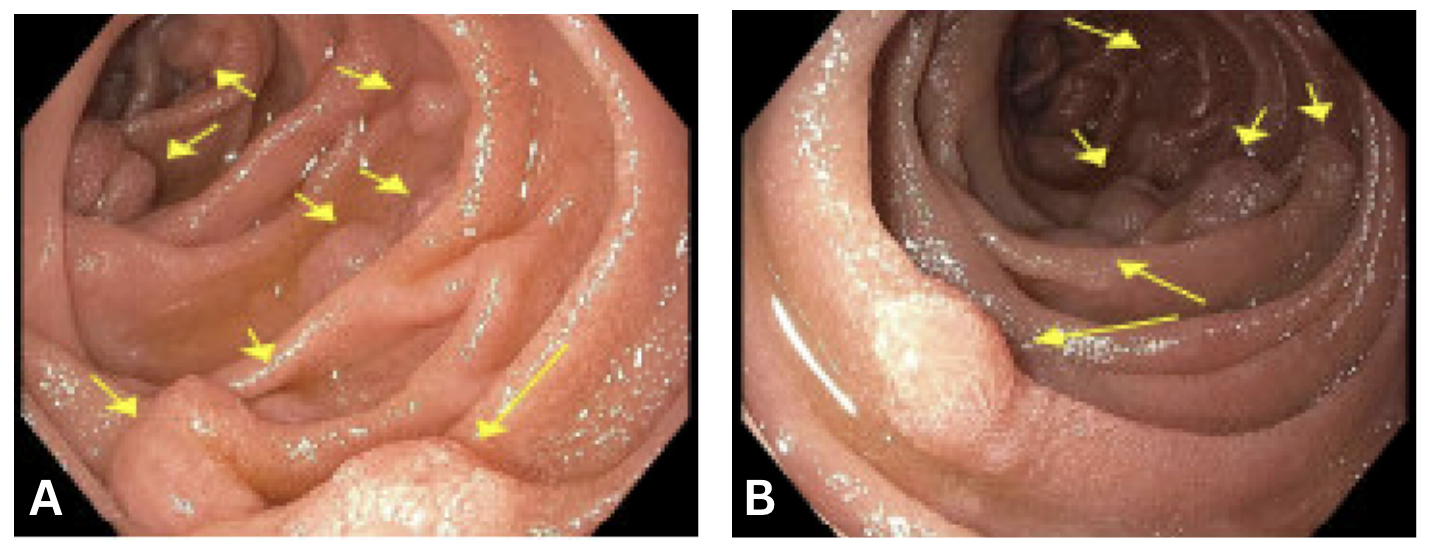
Figure: Image 1a and 1b: Esophagoduodenoscopy findings showing nodular changes and sessile polyps (yellow arrows) in the duodenum
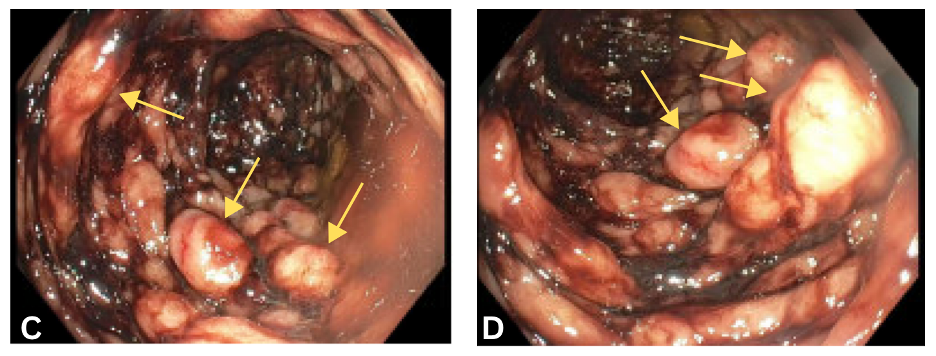
Figure: Image 2c and 2d: Colonoscopy findings showing diffuse areas of severely nodular and edematous mucosa (yellow arrows) with hematochezia in the rectum
Disclosures: Aishwarya Gatiganti indicated no relevant financial relationships. Husayn Ramji indicated no relevant financial relationships. John Bloch indicated no relevant financial relationships.
Aishwarya Gatiganti, MD1, Husayn F. Ramji, MD2, John M. Bloch, MD1. P3133 - An Unusual Cause of Hematochezia: Advanced Mantle Cell Lymphoma With Upper and Lower Endoscopic Findings, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")