University of Miami Miller School of Medicine at Holy Cross Hospital Fort Lauderdale, FL
Cinthia Reyes Cruz, MD, John Coleman, MD, Melaine Lanza, MD, Nemer Dabage-Forzoli, MD, Charles Hotte, MD University of Miami Miller School of Medicine at Holy Cross Hospital, Fort Lauderdale, FL Introduction: Meckel's diverticulum (MD) is a congenital anomaly of the gastrointestinal (GI) tract that presents as painless episodes of GI bleeding. It is the most common congenital abnormality of the small intestine, occurs in approximately 2% of the population. Although the diagnosis is confirmed with technetium-99m pertechnetate scans, it remains a challenging clinical entity.
Case Description/
Methods: 24-year-old male with history of anxiety who presented to the emergency department (ED) with a 3-day history of bright red blood per rectum, weakness and syncope accompanied by non-bloody, non-bilious vomiting. He had previously undergone esophagogastroduodenoscopy (EGD) and colonoscopy 10 and 5 years prior to the patient’s current hospital admission, respectively, due to similar GI bleeding episodes. This prior work-up was unrevealing.
Laboratory results on admission were significant for hemoglobin of 4.5. On presentation, sinus tachycardia was noted, and abdominal physical exam was unremarkable. He received intravenous fluids, pantoprazole, and packed red blood cell transfusions. He was monitored in the Intensive Care Unit. EGD, colonoscopy and video capsule endoscopy (VCE) were unremarkable and showed no identifiable etiology for the bleed. The patient had stopped bleeding by the time of these studies.
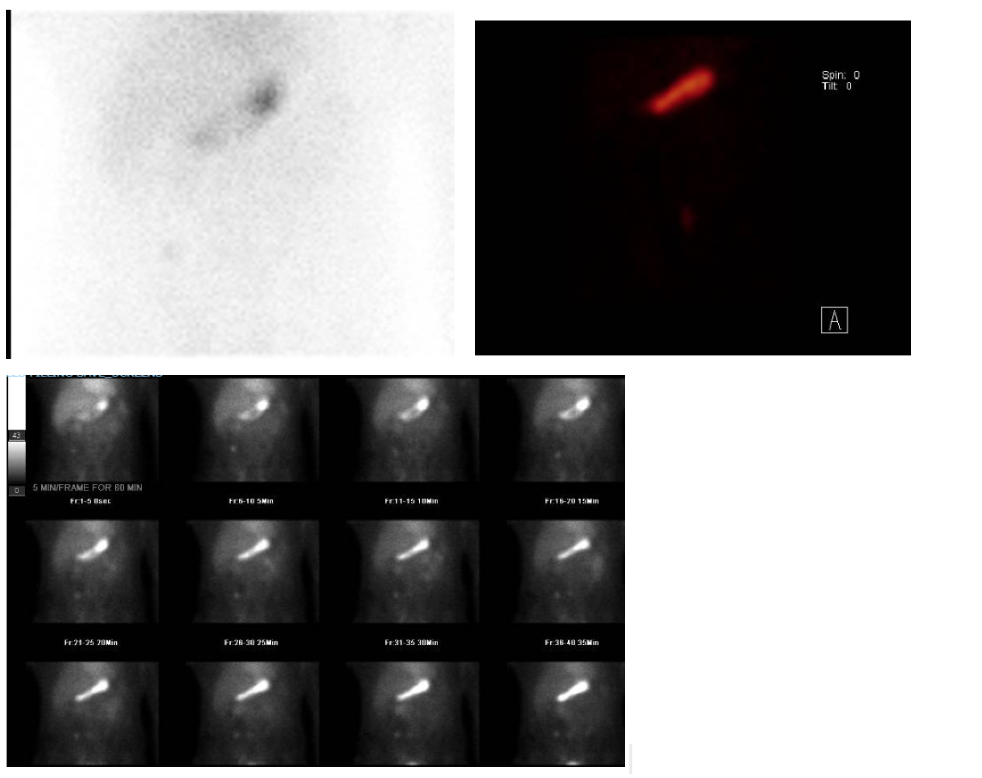
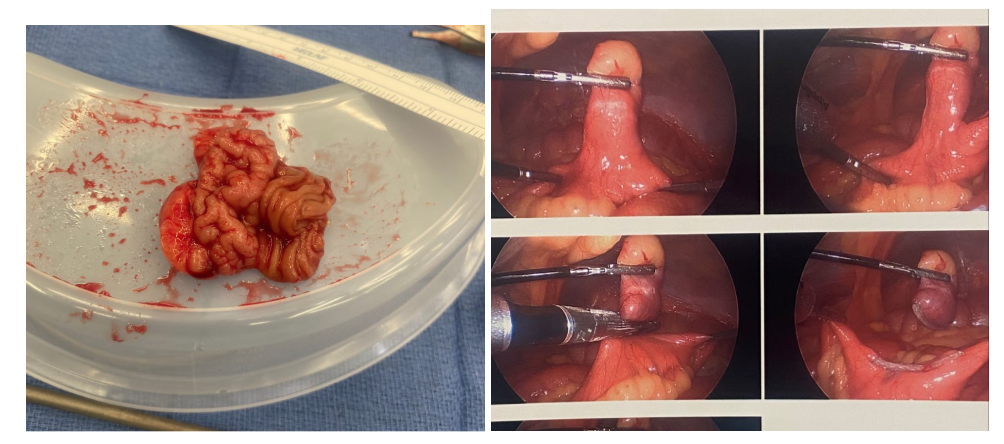
A Meckel scan was ordered given the patient's history of unexplained bleeding episodes. The results were ambiguous. There was mild initial tracer localization in the right lower quadrant, corresponding with the area near the ileocecal valve but there was no clear uptake suggesting ectopic parietal cells (Figure 1). Ultimately, the patient went for a laparoscopic resection of the MD, found at 90 cm from the ileocecal valve on the antimesenteric border of the terminal ileum (Figure 2). This confirmed the diagnosis and resolved the patient's symptoms without further episodes of bleeding. Discussion: This case highlights the complexity of diagnosing MD in patients presenting with obscure GI bleeding, especially when imaging results are inconclusive. In this case, endoscopy showed no signs of an active bleed, and VCE was negative. Despite ambiguous imaging results, high clinical suspicion and surgical exploration led to the correct diagnosis. We highlight the importance of considering MD in the differential diagnosis for young patients with recurrent GI bleeding, particularly in those without obvious findings on the endoscopic and imaging workup.
Figure: Figure 1. Meckel's scan results
Figure: Figure 2. Intraoperative photos of Meckel’s Diverticulum resection
Disclosures: Cinthia Reyes Cruz indicated no relevant financial relationships. John Coleman indicated no relevant financial relationships. Melaine Lanza indicated no relevant financial relationships. Nemer Dabage-Forzoli indicated no relevant financial relationships. Charles Hotte indicated no relevant financial relationships.
Cinthia Reyes Cruz, MD, John Coleman, MD, Melaine Lanza, MD, Nemer Dabage-Forzoli, MD, Charles Hotte, MD. P3122 - Challenging Imaging in the Diagnosis of Meckel's Diverticulum, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.