MedStar Georgetown University Hospital Washington, DC
Ade Waterman, MBChB, Adam Khalaf, MD, Lavannya Atri, MD, Mark Mattar, MD, Walid Chalhoub, MD MedStar Georgetown University Hospital, Washington, DC Introduction: Disseminated Gonococcal Infection (DGI) is an uncommon complication of Neisseria gonorrhoeae, seen in 0.5–3% of cases. It typically affects women under 40 and presents with arthritis-dermatitis syndrome. Gastrointestinal manifestations are exceedingly rare, and no prior reports describe DGI associated with new-onset inflammatory bowel disease (IBD).
Case Description/
Methods: A 25-year-old HIV-negative male with no autoimmune history presented with joint pain, body aches, and chest pain one week after hospitalization for DGI complicated by sepsis. Two months earlier, he was treated for urethral gonorrhea with IM ceftriaxone and oral cefixime. Persistent polyarthralgia led to NSAID initiation, while steroids were avoided due to infection risk. During admission, he developed watery diarrhea, hematochezia, abdominal pain, microcytic anemia, and a 10-lb weight loss. Stool studies for infection were negative. Labs showed ESR 129, CRP 121, calprotectin >3000, and positive lactoferrin. CTA abdomen/pelvis revealed nodular thickening and skip lesions in the colon and ileum. On readmission, colonoscopy revealed friable, nodular, erythematous mucosa in the cecum, hepatic flexure, and descending colon. Biopsies showed severe chronic active colitis with focal neutrophilic cryptitis, crypt microabscesses, ulceration, and granulation tissue. No dysplasia or granulomas were found. EBV LMP and CMV stains were negative. Discussion: To our knowledge, this is the first reported case of new-onset IBD in the context of DGI. While causality cannot be confirmed, N. gonorrhoeae may have triggered immune dysregulation and gut dysbiosis, unmasking Crohn’s disease. Management included antibiotic completion and referral for chronic IBD therapy. This case underscores the need to consider immune-mediated disease in patients with persistent GI symptoms after systemic infection.
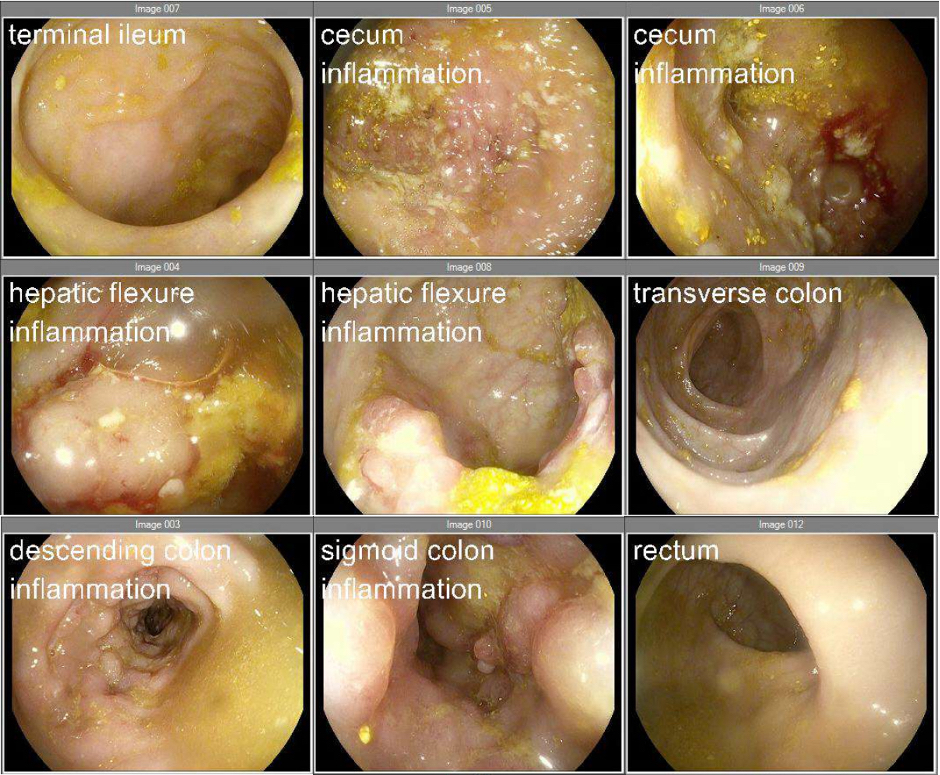
Figure: Figure 1. Images acquired during colonoscopy show abnormal patches of inflammation with friable, erythematous, and nodular mucosa at the following locations: Row 1 – Inflammation at the cecum extending into the ascending colon. Row 2 – Inflammation at the hepatic flexure extending into the proximal transverse colon. Row 3 – Inflammation at the descending colon extending into the sigmoid colon.
Disclosures: Ade Waterman indicated no relevant financial relationships. Adam Khalaf indicated no relevant financial relationships. Lavannya Atri indicated no relevant financial relationships. Mark Mattar: AbbVie – Consultant, Speakers Bureau. Celltrion – Speakers Bureau. Johnson & Johnson – Consultant, Speakers Bureau. Walid Chalhoub indicated no relevant financial relationships.
Ade Waterman, MBChB, Adam Khalaf, MD, Lavannya Atri, MD, Mark Mattar, MD, Walid Chalhoub, MD. P3362 - The Enteric Fallout of a Systemic STI: New-Onset Inflammatory Bowel Disease After Disseminated Gonococcal Infection, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")