Monday Poster Session
Category: IBD
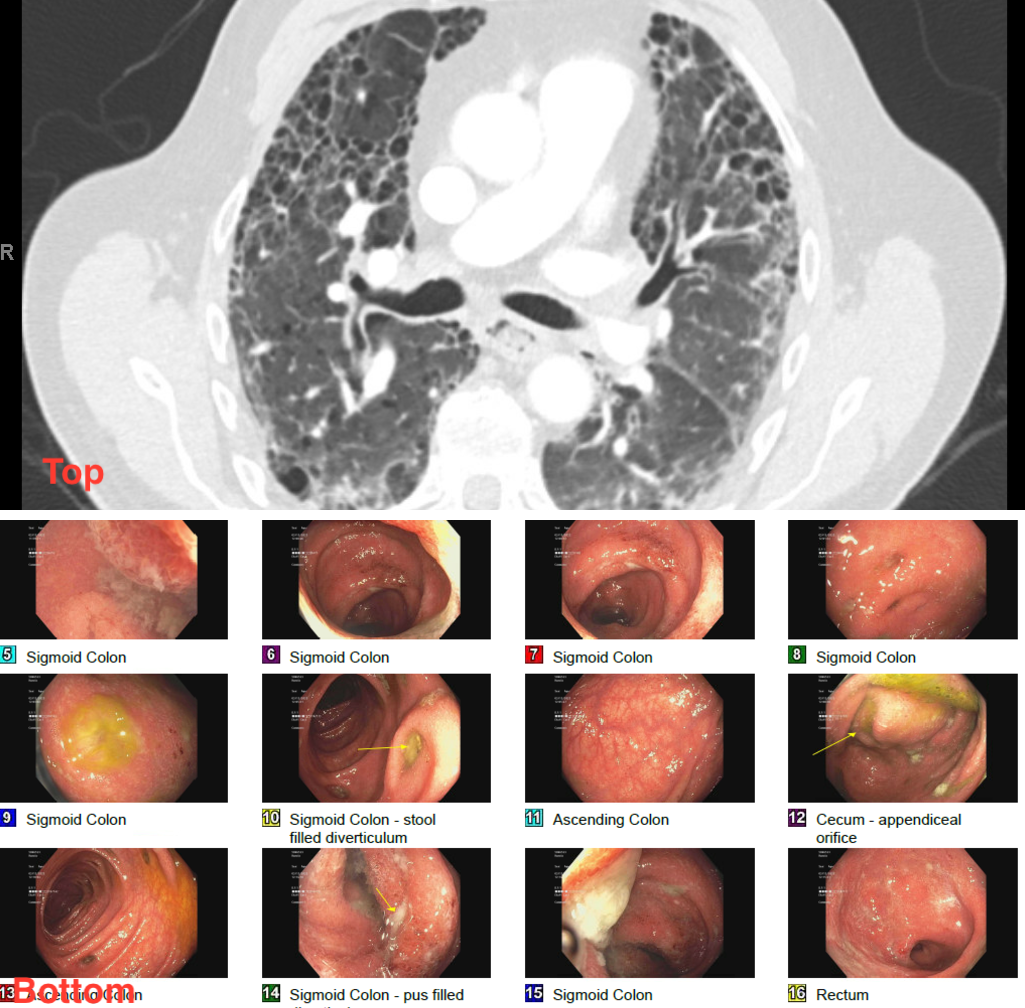
Ulcerative Colitis and ILD Complicated by Recurrent Enteric Infections: A Case of <i>C. difficile</i> and <i>C. perfringens</i> Bacteremia
 photo")
Ahmad Zain, MBBS (he/him/his)
Parkview Medical Center
Pueblo, CO