Wilfredo J.. Javier-Rojas, MD1, Alvin B.. Newman-Caro, DO1, Mamoon Ghellai, MD1, Vamsee Mupparaju, MD2, Sreekanth Chandrupatla, MD2, Siddharth Mathur, MD2, Yizhi Lin, DO1 1HCA Florida Blake Hospital, Bradenton, FL; 2HCA Florida Citrus Hospital, Inverness, FL Introduction: Upadacitinib is an immunosuppressant that selectively inhibits Janus Kinase 1 (JAK1). It may elevate the risk of opportunistic infections and viral reactivations. To date, no instances of upadacitinib-induced CMV viremia or pneumonitis in the presence of inflammatory bowel disease (IBD) have been reported in the literature.
Case Description/
Methods: The patient is a 59-year-old male with a medical history of ulcerative colitis (UC) managed with upadacitinib (on his 4th week of treatment), primary sclerosing cholangitis (PSC), polymyalgia rheumatica (PMR) managed with a stable, chronic dose of Prednisone and prostate cancer status post-brachytherapy, who presented with a 9-day history of persistent fever, chills, night sweats, shortness of breath, and a nonproductive cough. A computed tomography angiogram (CTA) of the chest revealed bilateral pneumatoceles, pulmonary densities, and a right-sided posterior subpleural density. A magnetic resonance cholangiopancreatography (MRCP) demonstrated diffuse irregular intrahepatic bile ducts, more prominent in the left lobe than the right, consistent with PSC. Additionally, there was colonic wall thickening, most prominent in the ascending colon, hepatic flexure, and proximal transverse colon, consistent with UC. A white blood cell (WBC) scan revealed an atypical infection in the bilateral lung bases. Subsequent complete blood count (CBC) with differential revealed 59% lymphocytes, suggesting a viral etiology. Inflammatory markers included an erythrocyte sedimentation rate (ESR) of 40 mm/hr, C-reactive protein (CRP) of 4.8 mg/dL, and stool calprotectin of 734 µg/g. Cytomegalovirus (CMV) DNA PCR was markedly elevated at 119,000 IU/mL, confirming CMV viremia. Valganciclovir was initiated. A Fiberoptic bronchoscopy with bronchoalveolar lavage (BAL) was performed. BAL cytology from the right lower lobe (RLL) showed rare cells with cytopathic changes suggestive of CMV, consistent with CMV pneumonitis. The patient’s symptoms continued to improve on valganciclovir. Discussion: CMV viremia and pneumonitis are recognized complications of upadacitinib therapy; however, these conditions are exceedingly rare in the context of IBD. The current literature on upadacitinib-induced CMV infections in IBD remains limited. As this case represents a novel presentation, further epidemiologic studies are warranted to assess the incidence, risk factors, and mechanisms of upadacitinib-induced CMV reactivation in IBD patients.
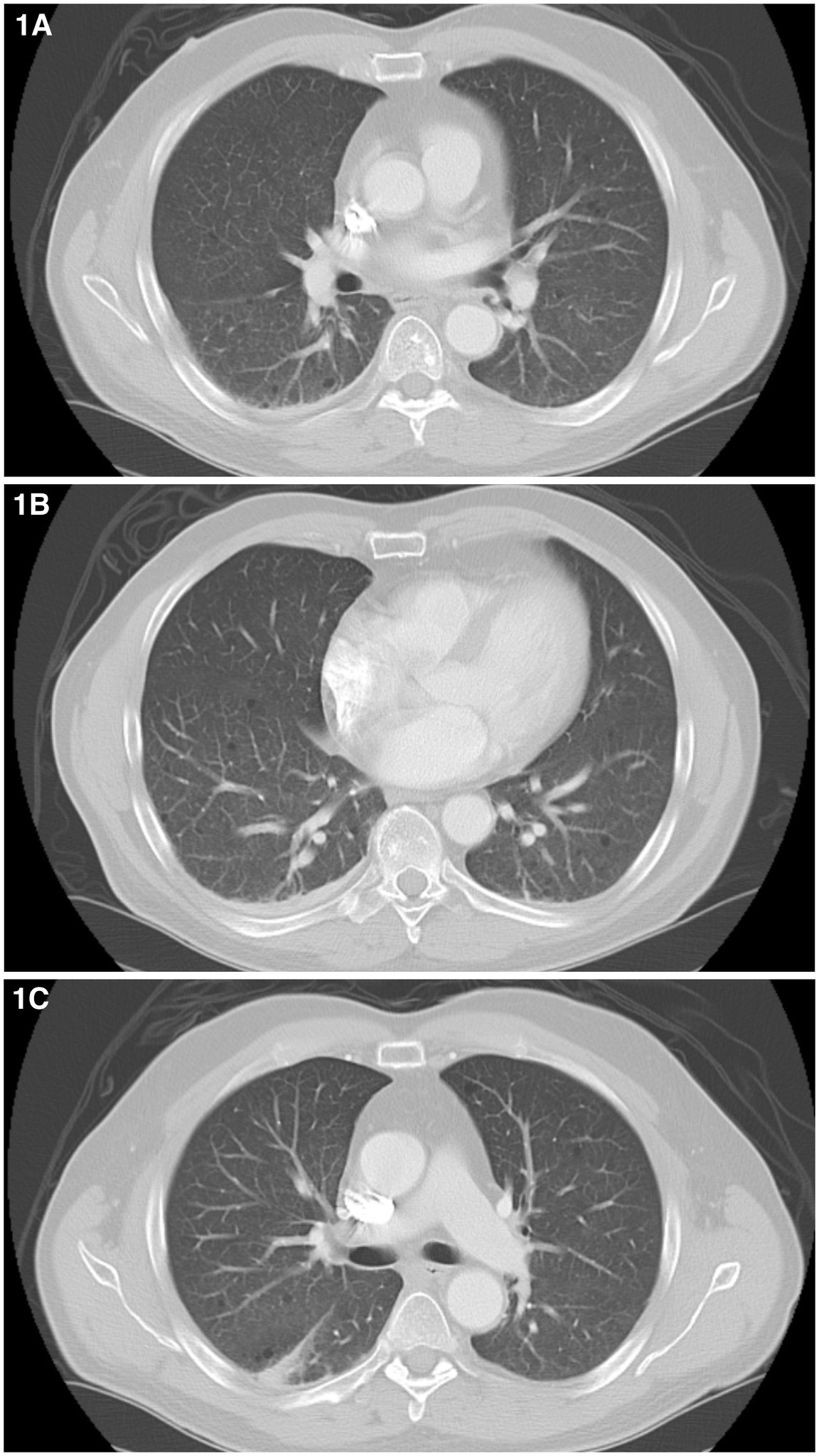
Figure: Figure 1A & 1B: Computed tomography angiogram (CTA) of the chest with bilateral pneumatoceles, findings consistent with an ongoing infectious process. Figure 1C: Computed tomography angiogram (CTA) of the chest revealing a posterior subpleural linear density in the superior segment of the right lower lobe (RLL). Bilateral pneumatoceles are also noted.
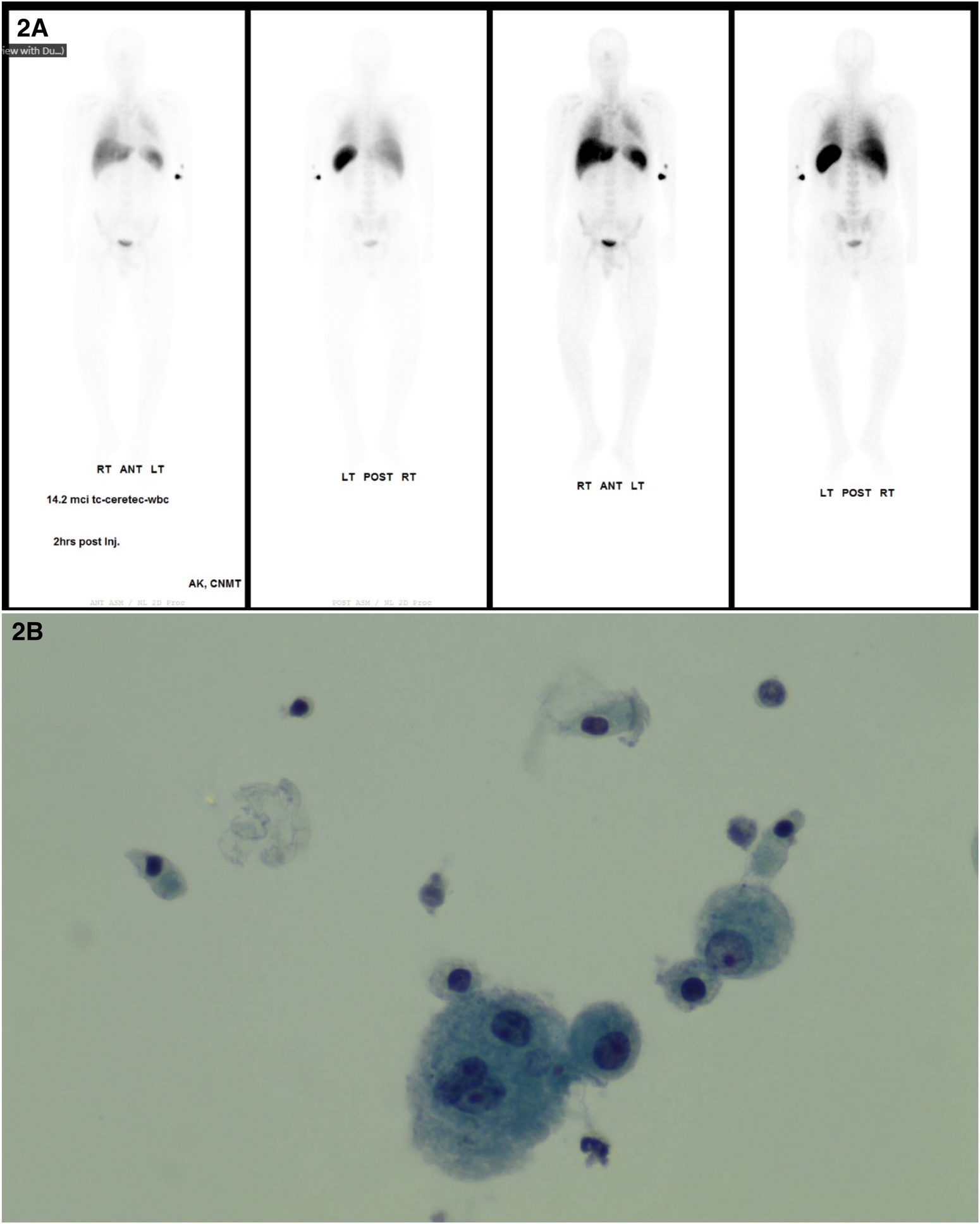
Figure: Figure 2A: White blood cell (WBC) scan showing abnormal diffuse bilateral lung activity, findings consistent with an occult atypical infection. Remainder of the tracer distribution is physiologic. Figure 2B: Cytology from right lower lobe (RLL). The slide shows rare cells with findings suggestive of CMV viral cytopathic effect, findings consistent with CMV infection.
Disclosures: Wilfredo Javier-Rojas indicated no relevant financial relationships. Alvin Newman-Caro indicated no relevant financial relationships. Mamoon Ghellai indicated no relevant financial relationships. Vamsee Mupparaju indicated no relevant financial relationships. Sreekanth Chandrupatla indicated no relevant financial relationships. Siddharth Mathur indicated no relevant financial relationships. Yizhi Lin indicated no relevant financial relationships.
Wilfredo J.. Javier-Rojas, MD1, Alvin B.. Newman-Caro, DO1, Mamoon Ghellai, MD1, Vamsee Mupparaju, MD2, Sreekanth Chandrupatla, MD2, Siddharth Mathur, MD2, Yizhi Lin, DO1. P3406 - First Reported Case of Upadacitinib-Induced CMV Viremia and Pneumonitis in Ulcerative Colitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Wilfredo J. Javier-Rojas, MD photo")