Stewart R. Malave, MD1, Erin Fannin, DO, MSPH2, Nathan Douthit, MD3 1East Alabama Medical Center, Auburn, AL; 2East Alabama Medical Center, Opelika, AL; 3Edward Via College of Osteopathic Medicine, Opelika, AL Introduction: Klebsiella pneumoniae primary liver abscess (KLA) is now recognized as the leading cause of community-acquired pyogenic liver abscess in many regions. Unlike traditional polymicrobial pyogenic liver abscesses, KLA is typically monomicrobial and can develop in the absence of hepatobiliary disease. Infection is most often due to hypervirulent serotypes, which have the potential to cause metastatic infections. Given the increasing prevalence and cryptogenic nature of this infection, clinicians must be aware of it. The following details a case of a healthy man who presented with a KLA and bacteremia without any identifiable inciting event.
Case Description/
Methods: A 35-year-old asian male with no significant PMH presented with body aches, chills, and right lower quadrant pain for a week prior to admission. Upon presentation, vitals showed tachycardia and high blood pressure. His lab work revealed alk-phos 158U/L, amylase 25U/L, lipase 18U/L, CRP 15mg/dL, and WBC 20.7 x10E3/mcL. A CT abdomen/pelvis w/ contrast showed clusters of small hypodensities in the right lobe of the liver, suggestive of abscesses. IV Zosyn was initiated, and infectious disease was consulted. Interventional radiology was consulted for CT aspiration; however, they were unable to drain the abscess. A liver biopsy and culture were performed instead. The routine culture identified K. pneumoniae, resistant to Ampicillin, for which antibiotics were changed to PO Augmentin and Levaquin. Upon further examination, physical, vitals and labs were unremarkable. The patient was discharged with Levaquin and Augmentin for 6 weeks with close follow-up, and a scheduled CT after the completion of antibiotics. Discussion: The clinical presentation of pyogenic liver abscesses is diverse, with common symptoms including fever, chills, and abdominal pain. Bloodwork in patients with hepatic abscesses can vary, with the most common laboratory findings including hypoalbuminemia, elevated liver enzymes, and leukocytosis. The diagnosis of hepatic abscesses is supported by ultrasonography and CT. Treatment for KLA includes antibiotics, often combined with percutaneous drainage. Isolates usually show resistance to ampicillin and penicillin, making third and fourth-generation cephalosporins the preferred first-line therapy. An extended course of antibiotics is recommended, lasting a total of 4-6 weeks. This case highlights the importance of early detection, proactive management, and awareness of antimicrobial resistance in the management of this condition.
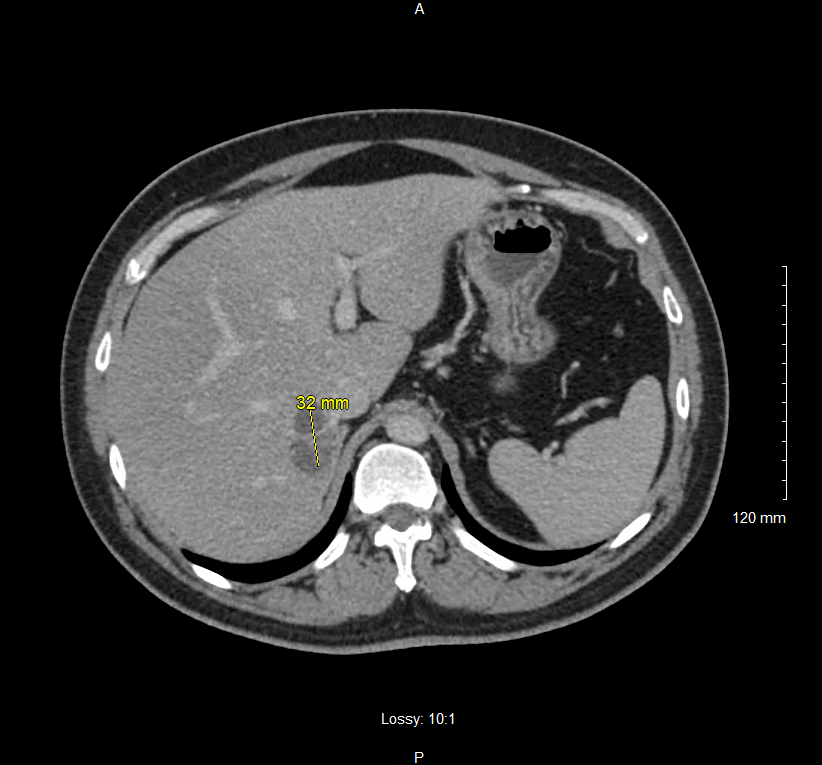
Figure: CT abdomen/pelvis with contrast showing clusters of small hypodensities in the Right Lobe of the Liver. Smaller collection measuring about 3cm in maximal diameter.
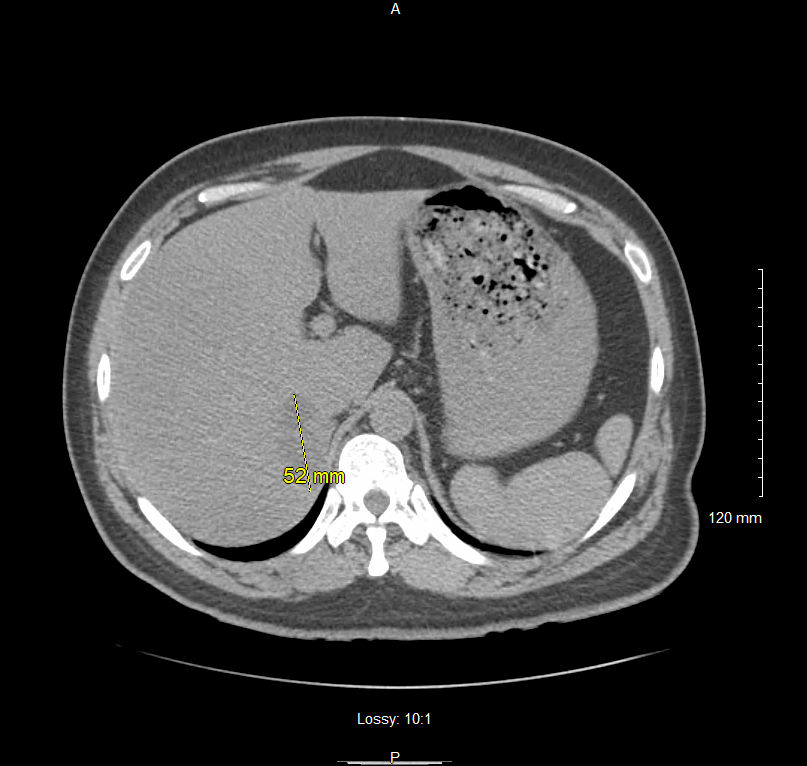
Figure: CT abdomen/pelvis with contrast showing clusters of small hypodensities in the Right Lobe of the Liver. Larger collection measuring about 5cm in maximal diameter.
Disclosures: Stewart Malave indicated no relevant financial relationships. Erin Fannin indicated no relevant financial relationships. Nathan Douthit indicated no relevant financial relationships.
Stewart R. Malave, MD1, Erin Fannin, DO, MSPH2, Nathan Douthit, MD3. P3490 - A Case of <i>K. pneumoniae</i> Primary Liver Abscess (KLA) in a Healthy Immunocompetent Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")