KIMS Savera hospital Anantapur, Andhra Pradesh, India
Dinesh Muthuluru, MD, DrNB, MNAMS1, Manoj Kumar Sahu, MD, DM2, Akash Anand Dobhada, MD, DrNB3, Sonit Bhusan Pattnaik, MSc2 1KIMS Savera hospital, Anantapur, Andhra Pradesh, India; 2Kalinga Institute of Medical Sciences, Bhubaneswar, Orissa, India; 3Apollo Hospital, Bhubaneswar, Orissa, India Introduction: The Ampulla of Vater typically lies in the posteromedial wall of the duodenum's second part. We report a rarecase of an ectopic ampulla in the pyloric canal, complicated by a 2 cm choledocholithiasis, successfully managed via endoscopic intervention.
Case Description/
Methods: A 65-year-old male, with no comorbidities, presented to our clinic with 5 days of abdominal pain, jaundice and 4 days of fever and chills. Labs showed total bilirubin 4.29 mg/dL, direct 2.7 mg/dL, SGOT 64 U/L, SGPT 108 U/L, ALP 188 U/L, TLC 14.83 x 10^9/L. Ultrasound confirmed choledocholithiasis; MRCP showed mild CBD dilation and a stone. Initial ERCP with a side-viewing duodenoscope failed to locate the ampulla. A forward-viewing endoscope revealed it in the pyloric canal, facing the stomach, with two slit-like openings. ERCP using a colonoscope achieved CBD cannulation. Cholangiogram showed a hook-shaped, dilated CBD with a 2 cm mid-CBD stone. Sphincteroplasty to 15 mm and balloon sweeps failed to remove the stone. A plastic double-pigtail stent was placed, and the patient was discharged, advised to follow up after cholangitis improved, with plans for cholangioscopy or lithotripsy. Three weeks later, repeat ERCP post-stent removal showed a cylindrical filling defect (< 1 cm diameter) in the mid-CBD. The stone was extracted via balloon with careful maneuvering, avoiding cholangioscopy or lithotripsy. He was discharged stable. Discussion: Ectopic Ampulla of Vater is rare, often in the duodenal bulb or pylorus, per limited studies. It may stem from embryogenic defects or ulcers/strictures pulling the ampulla proximally. Peng et al.’s 23-year study of 6,133 ERCP cases noted a 0.13% incidence. Saritas et al. reported 10 cases, mostly in the duodenal bulb, one in the pyloric canal, with cholangitis and hook-shaped CBD dilation common. Management used sphincteroplasty and balloons or baskets, sometimes surgery. Our case had a dilated CBD, large stone, and cholangitis. Initial ERCP failed, but stenting reshaped the stone to a cylindrical form (< 1 cm), aiding removal. We hypothesize de novo stone formation in CBD due to altered mid- and distal CBD anatomy, causing bile stasis and sludge buildup. The stent likely scaffolded the soft calculus, easing extraction. Choledocholithiasis with ectopic Ampulla of Vater is rare and challenging. A colonoscope or gastroscope may suit ERCP for altered anatomy. Stenting to ease cholangitis, followed by repeat ERCP with tools like baskets or lithotripsy, can extract stones, avoiding surgery.
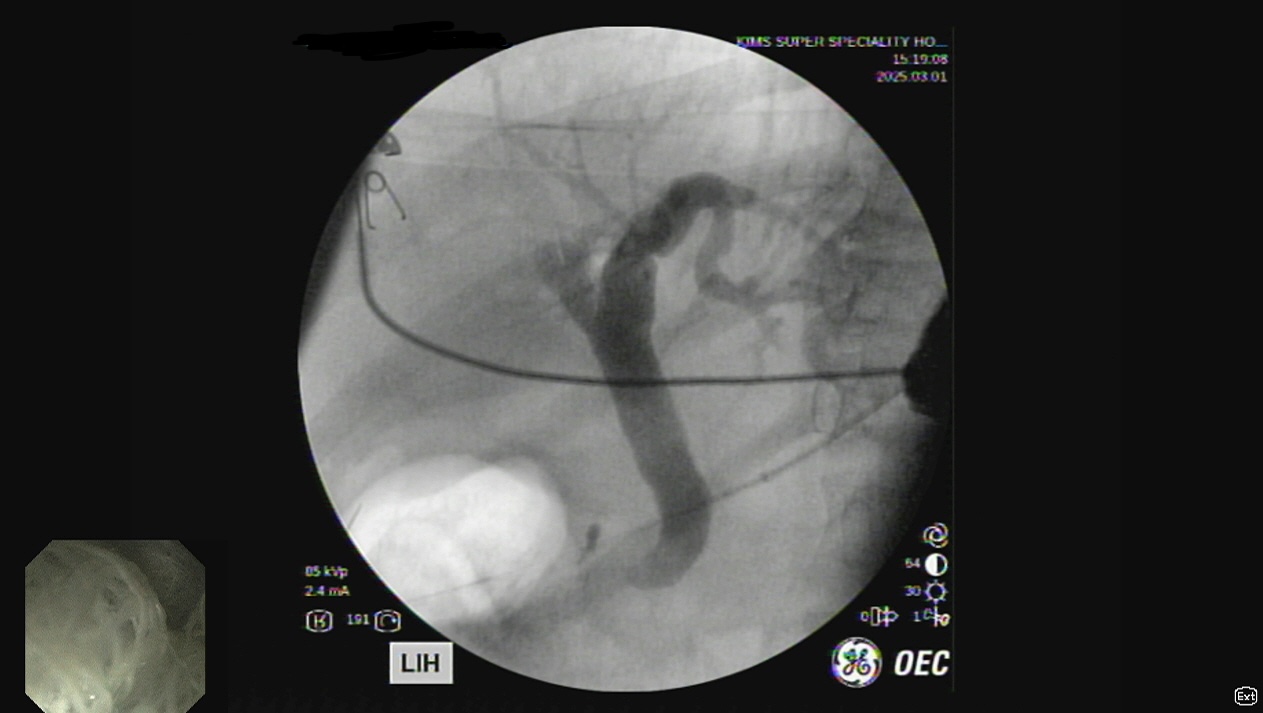
Figure: Cholangiogram showing hook shaped CBD at distal end
Figure: Ectopic ampulla in pylorus with seperate biliary and pancreatic openings
Disclosures: Dinesh Muthuluru indicated no relevant financial relationships. Manoj Kumar Sahu indicated no relevant financial relationships. Akash Anand Dobhada indicated no relevant financial relationships. Sonit Bhusan Pattnaik indicated no relevant financial relationships.
Dinesh Muthuluru, MD, DrNB, MNAMS1, Manoj Kumar Sahu, MD, DM2, Akash Anand Dobhada, MD, DrNB3, Sonit Bhusan Pattnaik, MSc2. P3560 - From Pyloric Surprise to Endoscopic Success: Managing Ectopic Ampulla of Vater and Large Choledocholithiasis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.