P3552 - Real-World Variation in Time to EUS and Treatment After Imaging-Detected Pancreatic Mass: A Multi-Center Comparison of Academic and Non-Academic Institutions
University of Central Florida, HCA Healthcare GME Gainesville, FL
Award: ACG Presidential Poster Award
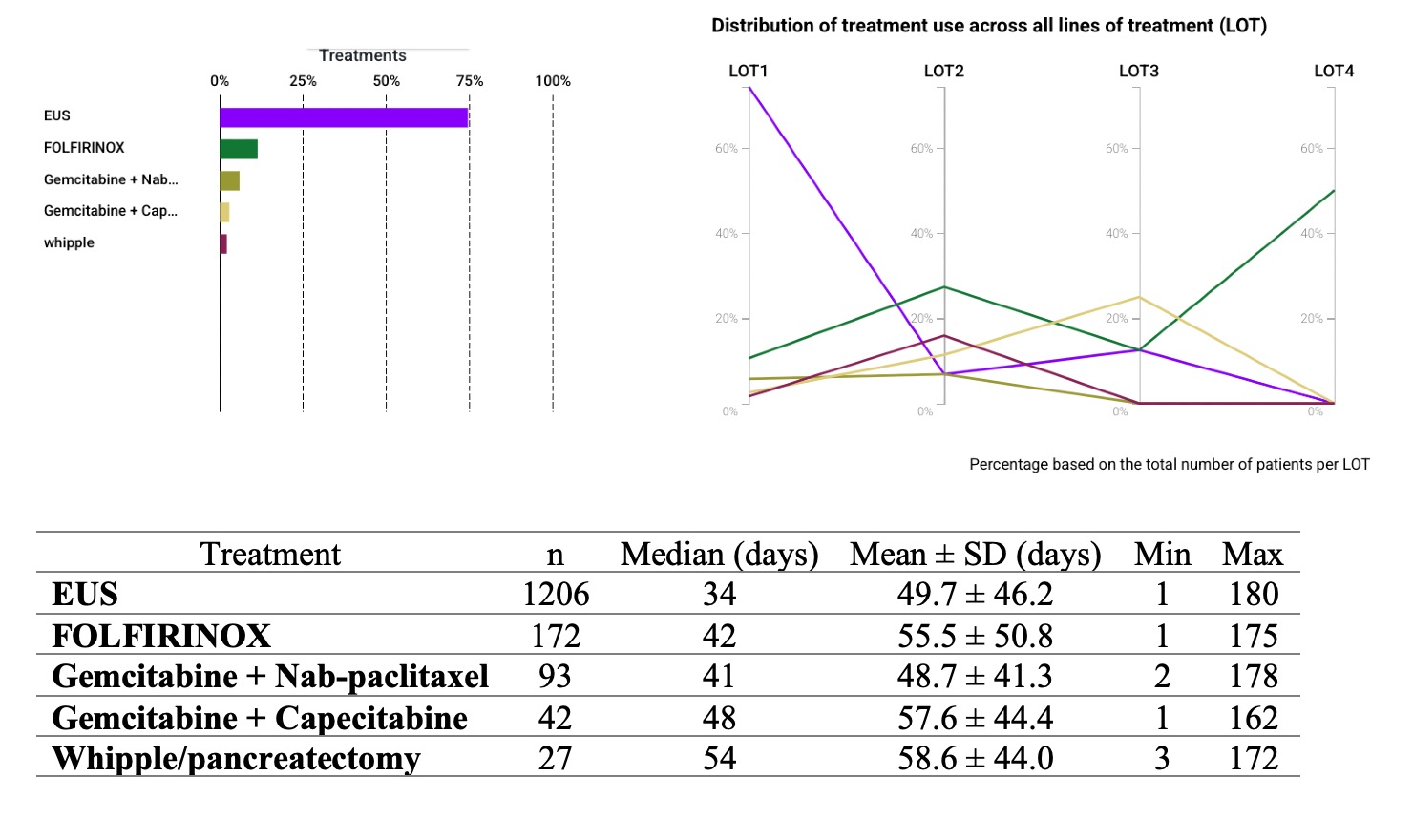
Mohammad Abuassi, MD1, Mahmoud Y. Madi, MD2, Ashraf Almomani, MD3, Tony Brar, MD4, Yaseen Perbtani, DO1 1University of Central Florida, HCA Healthcare GME, Gainesville, FL; 2University of Texas at Austin Dell Medical School, Austin, TX; 3Cleveland Clinic Florida, Weston, FL; 4University of Central Florida, Gainesville, FL Introduction: Endoscopic ultrasound (EUS) is essential for diagnosing suspected pancreatic cancer and guiding timely treatment. However, real-world data describing delays between imaging-detected pancreatic abnormalities and subsequent interventions remain limited, particularly across varied healthcare settings. Methods: We conducted a retrospective cohort study using the TriNetX US Network, a database of de-identified records from 65 healthcare organizations. Adults with imaging-detected pancreatic abnormalities between 2020-2024 were included. Eligibility required diagnostic abdominal imaging (CPT: 1010537 or 1010520) + abnormal findings (ICD-10: R93), and exclusion of patients with prior EUS or a pancreatic cancer diagnosis (ICD-10: C25) before the index date. A same-day pancreatic disorder code (ICD-10: K86.x) was used to approximate mass detection via imaging. We used TriNetX’s Treatment Pathways tool to identify patients who underwent EUS, chemotherapy, or Whipple procedure within 180 days of the index date. Patients without a documented treatment pathway were excluded. A subgroup analysis compared time to EUS between academic and non-academic institutions. Results: A total of 1,624 patients met inclusion criteria. The median time from index to EUS (n = 1,206) was 34 days (mean: 49.7 ± 46.2). Chemotherapy was administered to 307 patients (18.9%), serving as a proxy for pancreatic malignancy. Median time to treatment was 42 days for FOLFIRINOX (n = 172; mean: 55.5 ± 50.8), 41 days for Gemcitabine + Nab-paclitaxel (n = 93; mean: 48.7 ± 41.3), and 48 days for Gemcitabine + Capecitabine (n = 42; mean: 57.6 ± 44.4). Patients who got Whipple resection (n = 27) had a median time to surgery of 54 days (mean: 58.6 ± 44.0). In subgroup analysis, patients at academic centers (n = 829) had a longer median time to EUS than those at non-academic centers (n = 377) 38 vs. 31 days (p = 0.014). Academic sites showed early clustering in some cases but greater overall variability, while non-academic centers demonstrated more consistent timing. Discussion: This multi-center analysis reveals significant delays from imaging-detected pancreatic abnormalities to diagnostic and therapeutic interventions. Academic centers offered early EUS access for some but showed greater variability and longer delays, likely due to higher demand and referrals. Non-academic centers had shorter, more consistent timelines. Findings highlight the need for standardized pathways to ensure timely care in suspected pancreatic cancer.
Figure: Utilization and timing of interventions following imaging-detected pancreatic abnormalities. (Left) Bar graph showing overall treatment frequencies, with EUS representing the most commonly performed intervention. (Right) Line chart illustrating treatment distribution across lines of therapy (LOT), with EUS predominantly used in LOT1, while FOLFIRINOX and other chemotherapies increase in later lines. Bottom panel displays the number of patients and timing metrics, including median, mean, and standard deviation, for each intervention from the index diagnosis.
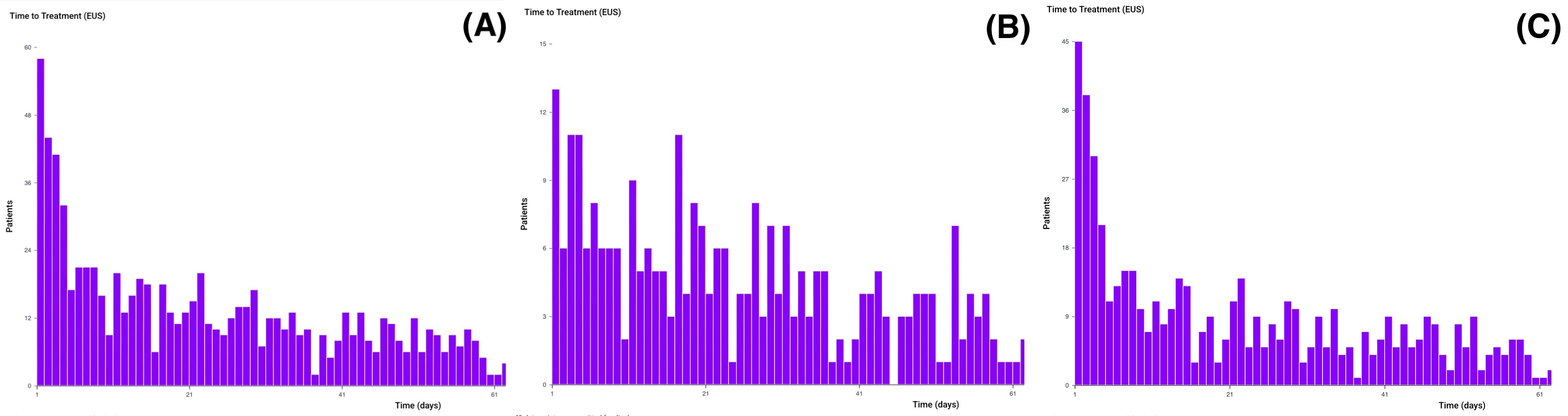
Figure: Time to endoscopic ultrasound (EUS) following imaging-detected pancreatic abnormalities. The overall cohort (Panel A) shows a right-skewed distribution, with most EUS procedures occurring within 30 days. Non-academic centers (Panel B) demonstrate a more concentrated and timely distribution (median 31 days), while academic centers (Panel C) show greater variability and prolonged delays (median 38 days). The difference was statistically significant (p = 0.014)
Disclosures: Mohammad Abuassi indicated no relevant financial relationships. Mahmoud Madi indicated no relevant financial relationships. Ashraf Almomani indicated no relevant financial relationships. Tony Brar indicated no relevant financial relationships. Yaseen Perbtani indicated no relevant financial relationships.
Mohammad Abuassi, MD1, Mahmoud Y. Madi, MD2, Ashraf Almomani, MD3, Tony Brar, MD4, Yaseen Perbtani, DO1. P3552 - Real-World Variation in Time to EUS and Treatment After Imaging-Detected Pancreatic Mass: A Multi-Center Comparison of Academic and Non-Academic Institutions, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")