Joanna Yuen, DO, MA1, Ruona Ebiai, MD1, Jasmine McNair, MD1, Sameera Shuaibi, MD1, Patt Panuncillon, DO2, Ricardo David Espinosa, MD1, Paula Cacioppo, MD3, Adil Memon, MD4, Mariana Zapata, MD1, Shobha Joshi, MD1 1Ochsner Health Clinic Foundation, New Orleans, LA; 2Ochsner Health Clinic Foundation, Pearland, TX; 3Ochsner Medical Center, New Orleans, LA; 4Ochsner Clinic Foundation, New Orleans, LA Introduction: Hepatopulmonary syndrome (HPS) is a well-described, but significant complication of cirrhosis. It is relatively uncommon with a 10-30% occurrence rate. Cirrhosis is a rare manifestation of sarcoidosis. Here we describe a case of severe HPS in a patient with known sarcoidosis and newly diagnosed cirrhosis.
Case Description/
Methods: A 63-year-old woman with a history of tobacco use and sarcoidosis, diagnosed by liver biopsy 20 years prior, presented with chronic, worsening hypoxia and dyspnea on exertion. She had finger clubbing and an oxygen saturation of 70%, requiring 15 L of high flow nasal cannula.
Labs were notable for polycythemia with a hemoglobin of 21 and hypoxemia with pH 7.370, partial pressure of carbon dioxide 38, and partial pressure of oxygen (PaO2) 45. Chest computed tomography (CT) demonstrated interstitial fibrosis and dilatation of pulmonary vasculature in bilateral lower lung zones. CT angiography showed numerous dilated venous structures in bilateral lower lobes, suggestive of varices, and hepatic steatosis. Transthoracic echocardiogram showed extra-cardiac shunting without pulmonary hypertension. Liver ultrasound showed newly discovered nodular morphology consistent with cirrhosis, and cardiac positron emission tomography was negative for cardiac sarcoidosis.
Upon discussion with Lung Transplant, the degree of hypoxemia was determined to not be consistent with sarcoid-associated interstitial lung disease. Instead, findings were thought to be due to HPS given her newly diagnosed cirrhosis, extra-cardiac shunting, and persistent PaO2 of less than 50 on room air. Cirrhosis was thought to be of sarcoid, with possible metabolic dysfunction-associated steatotic liver disease, etiology. Liver transplant was deferred at that time based on questionable benefit, high risk, and a stable Model for End-Stage Liver Disease score of 12. Discussion: HPS severity is determined by arterial oxygen content and the difference in alveolar and arterial oxygen content. Criteria for the most severe form of HPS includes a PaO2 less than 50 and an alveolar-arterial oxygen gradient greater than 15 on room air, as demonstrated by this patient. However, profound hypoxemia in HPS is uncommon and tends to be seen in more advanced cases. Due to the rarity of significant hepatic manifestations in sarcoidosis, HPS is an underrecognized complication of chronic liver disease in this setting. Further understanding is needed to better classify the differences of HPS from that of other causes.
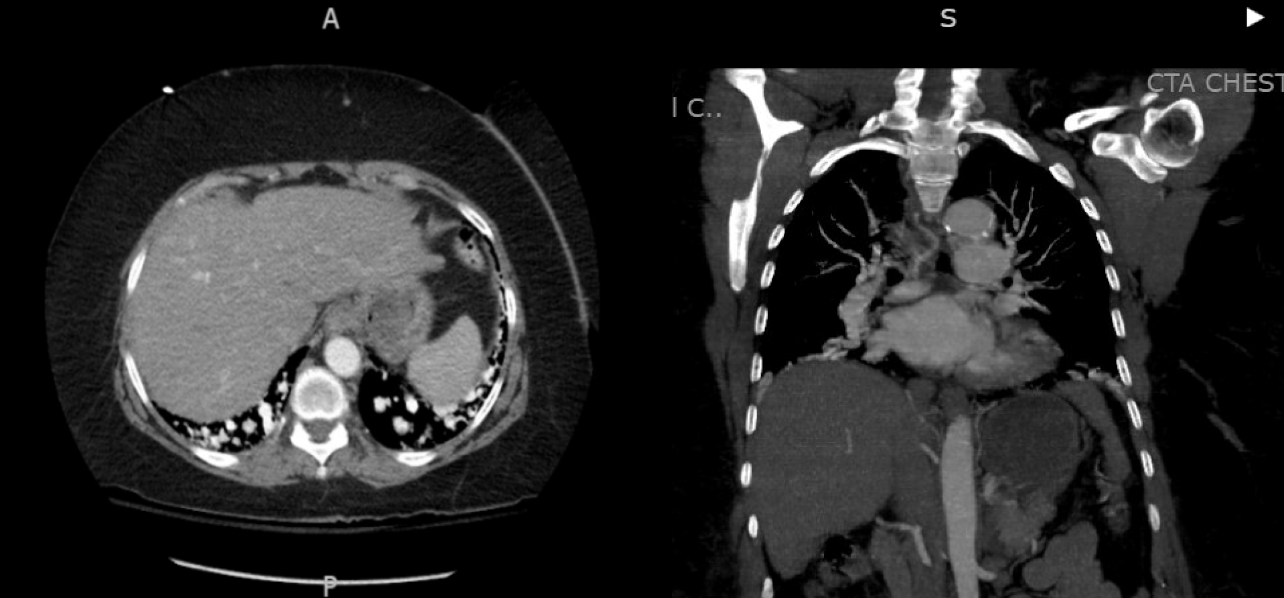
Figure: Figure 1. CT angiogram of the chest demonstrating moderate-to-severe symmetric, diffuse dilatation of predominantly the distal basilar branches of the pulmonary veins which extend to the pleural surfaces bilaterally, as can be seen in the setting of hepatic pulmonary syndrome, and diffuse hepatic steatosis.
Disclosures: Joanna Yuen indicated no relevant financial relationships. Ruona Ebiai indicated no relevant financial relationships. Jasmine McNair indicated no relevant financial relationships. Sameera Shuaibi indicated no relevant financial relationships. Patt Panuncillon indicated no relevant financial relationships. Ricardo David Espinosa indicated no relevant financial relationships. Paula Cacioppo indicated no relevant financial relationships. Adil Memon indicated no relevant financial relationships. Mariana Zapata indicated no relevant financial relationships. Shobha Joshi indicated no relevant financial relationships.
Joanna Yuen, DO, MA1, Ruona Ebiai, MD1, Jasmine McNair, MD1, Sameera Shuaibi, MD1, Patt Panuncillon, DO2, Ricardo David Espinosa, MD1, Paula Cacioppo, MD3, Adil Memon, MD4, Mariana Zapata, MD1, Shobha Joshi, MD1. P3958 - Hepatopulmonary Syndrome: A Case of Severe Pulmonary Vascular Dilatation in Newly Diagnosed Sarcoid Cirrhosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")