Riya Gupta, MBBS1, David J. Bartlett, MD1, Victor Chedid, MD, MSc1, Moataz Aboeldahb, MBBCh2, Xiao Jing Wang, MD1 1Mayo Clinic, Rochester, MN; 2Mayo Clinic College of Medicine and Science, Rochester, MN Introduction: CT enterography (CTE) is optimized for small bowel evaluation. According to the American College of Radiology (ACR) appropriateness criteria, “usually appropriate” indications for CTE include evaluations for Crohn’s disease (suspected, exacerbation and surveillance), pouchitis and proctitis, nonvariceal upper gastrointestinal (GI) bleed with negative endoscopy, and intermittent/low-grade small bowel obstruction. Beyond these, CTE is frequently ordered for clinical evaluation of chronic abdominal pain, diarrhea, and other GI symptoms. CTE involves exposure to ionizing radiation, use of intravenous contrast, cost, and potential patient discomfort. This study evaluates whether CTE performedfor “usually appropriate” indications is associated with a higher diagnostic yield and greater impact on clinical management compared to other indications.
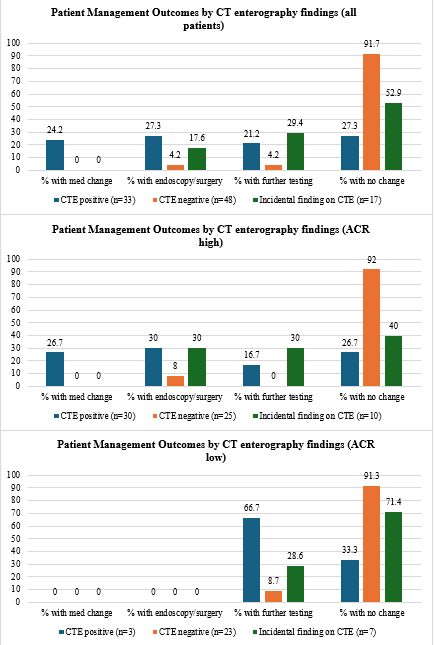
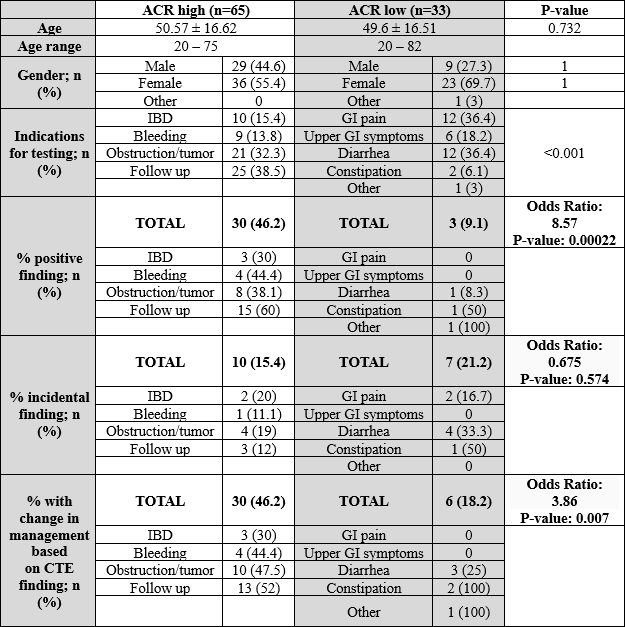
Methods: We reviewed 98 adult patients who underwent CTE over 4 weeks at a tertiary care center. CTEs were categorized as “ACR high” if indications were deemed “usually appropriate” by ACR, or “ACR low” if not. CTE results were extracted from radiology reports and classified as positive, negative, or incidental based on if they had any finding for the test indication. Management changes were recorded (medication change, endoscopy/surgery, further testing, or no change). Odds ratios and chi-square tests compared outcomes between groups. Results: Of 98 patients, 65 (66.3%) had ACR high indications and 33 (33.7%) had ACR low indications. Positive findings occurred more frequently in the ACR high group (46.2%) compared to the ACR low group (9.1%) (OR 8.57, p< 0.001). Change in management occurred in 46.2% of ACR high CTEs vs. 18.2% of ACR low (OR 3.86, p=0.007). Incidental findings were similar between groups (15% vs. 21%, p=0.574). Among ACR high CTEs, 26.7% led to medication changes and 30% to endoscopic or surgical intervention. In contrast, ACR low CTEs rarely resulted in intervention and most (91.3%) did not change management. Discussion: CTE performed in accordance with ACR appropriateness criteria yielded significantly higher diagnostic and therapeutic value than those performed for ACR low appropriateness indications. ACR low CTEs often do not impact management (though may provide reassurance) and may contribute to unnecessary radiation and increased costs. Appropriateness criteria can be a helpful clinical decision support tool in choosing imaging options for GI symptoms work up and setting patient expectations for findings.
Figure: Demographical population of patients undergoing CT enterography with results
Figure: Patient Management Outcome by CT enterography findings
Disclosures: Riya Gupta indicated no relevant financial relationships. David J. Bartlett indicated no relevant financial relationships. Victor Chedid: Pfizer – Grant/Research Support. Takeda – Consultant. Moataz Aboeldahb indicated no relevant financial relationships. Xiao Jing Wang indicated no relevant financial relationships.
Riya Gupta, MBBS1, David J. Bartlett, MD1, Victor Chedid, MD, MSc1, Moataz Aboeldahb, MBBCh2, Xiao Jing Wang, MD1. P4029 - Yield and Clinical Impact of CT Enterography by Study Indication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.