University of Pittsburgh Medical Center Pittsburgh, PA
Thomas Gonzales, MD, Varun Jain, MD, Sultan Mahmood, MD University of Pittsburgh Medical Center, Pittsburgh, PA Introduction: Intramural duodenal hematoma (DH), a rare pathology primarily associated with blunt trauma in pediatrics and young adults or with spontaneous bleeding due to anticoagulation usage, can cause a bulge into the intraluminal space.1,2 Osmotic fluid shifts may increase the size of the DH leading to gastric outlet obstruction (GOO).1,2 Here, we present the case of a 62-year-old male with a DH causing GOO secondary to pancreatic adenocarcinoma.
Case Description/
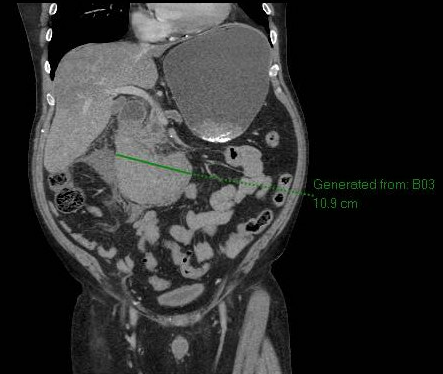
Methods: A 62-year-old male presented with a 1-day history of abdominal pain, decreased flatus, and non-bilious emesis that transitioned to hematemesis. CT revealed an 11 cm intramural DH causing GOO as well as a 2.1 cm pancreatic head lesion causing upstream ductal dilatation (Figure 1). Esophagogastroduodenoscopy found a severe extrinsic deformity in the duodenal bulb and in the second portion of the duodenum, consistent with hematoma (Figure 2). Followup endoscopic ultrasound showed a 2.3 x 2.2 cm hypoechoic irregular mass in the pancreatic head. Biopsy and elevated CA 19-9 confirmed pancreatic adenocarcinoma. Staging CT scans did not reveal metastases. He underwent gastrojejunostomy bypass. Discussion: DH caused by pancreatic adenocarcinoma is a rare etiology of GOO. Multiple theories for the pathophysiology of pancreatic cancer leading to DH exist including pancreatic enzymes causing tissue degradation, vascular erosion, and hematoma development.3CT scans, the diagnostic modality of choice for adults, characteristically show a duodenal mass with fluid density indicative of blood.4Since DHs typically self-resolve, treatment focuses on conservative management with bowel decompression and rest monitored with CT scans.1 Consistent with protocol, the patient was treated conservatively. However, the etiology of pancreatic adenocarcinoma leading to DH and GOO supports surgery.1
This case highlights the importance of a broad differential diagnosis for GOO, including rare causes such as DH. Etiology dictates treatment.
1. Pérez-Rubio et al. Intramural duodenal hematoma: diagnosis and management of a rare entity. 2023; 515-518
2. Diniz-Santos et al.. Duodenal hematoma following endoscopic duodenal biopsy: a case report and review of the existing literature.2006; 39-42
3. Kumar et al.. Spontaneous Intramural Duodenal Hematoma: A Rare Complication of Pancreatitis. 2020
4. Niehues et al. Intramural duodenal hematoma: clinical course and imaging findings. 2019; 1-8
Figure: Figure 1. CT abdomen/pelvis showing an 11 cm duodenal intramural hematoma with gastric outlet obstruction.
Figure: Figure 2. EGD image of severe extrinsic deformity in the second portion of the duodenum.
Disclosures: Thomas Gonzales indicated no relevant financial relationships. Varun Jain indicated no relevant financial relationships. Sultan Mahmood indicated no relevant financial relationships.
Thomas Gonzales, MD, Varun Jain, MD, Sultan Mahmood, MD. P4095 - An Unsual Case of Gastric Outlet Obstruction: Duodenal Hematoma from Pancreatic Cancer Infiltration, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")