Jefferson Einstein Hospital/Thomas Jefferson University Philadelphia, PA
Christie Polycarpe, DO, Nandakumar Mohan, DO, Oluwanifemi Balogun, MD, Shyam Patel, MD Jefferson Einstein Hospital/Thomas Jefferson University, Philadelphia, PA Introduction: Isolated inflammation of the terminal portion of the ileum is most commonly associated with underlying Crohn’s disease, certain medications such as NSAIDs, infection, or malignancy. Here, we present a rare case of acute ileal diverticulitis with enterolith as a cause of isolated terminal ileitis in a 55-year-old male who presented with generalized abdominal pain.
Case Description/
Methods: A 55-year-old male with past medical history significant for kidney transplant in 2024 for ESRD, partial left colectomy with colorectal anastomosis for recurrent diverticulitis, and GERD, presented for complaint of generalized abdominal pain for one week. He initially presented to an outside hospital, where he underwent a CT scan without contrast that revealed inflammatory fat stranding surrounding the terminal ileum, consistent with terminal ileitis. Patient also underwent EGD at outside hospital that showed gastritis, normal esophagus, and normal duodenum. He was referred to our hospital, for continuity of care in setting of his kidney transplant history. Upon presentation to our center, he was afebrile and hemodynamically stable. Labs were notable for mild leukocytosis to 11.3. Repeat CT scan without contrast demonstrated fat stranding of the terminal ileum and mesenteric edema suggestive of terminal ileitis, as well as multiple subcentimer hyperdense calcifications within the lumen of the terminal ileum and cecum, which may represent obstructive enterolith. Patient symptomatically improved with conservative management of IV antibiotics, bowel regimen, and IV fluids. Gastroenterology recommended MRCP to rule out cholelithiasis and biliary-enteric fistula as cause of enterolith, it was later negative for these findings. Patient was recommended for outpatient colonoscopy for biopsy of terminal ileum. Discussion: Small bowel diverticula typically occur in the duodenum, and are generally an incidental finding in asymptomatic patients. Acute diverticulitis of the ileum is uncommon, with a reported incidence of less than 10%. Small bowel enteroliths can originate from primary intestinal hypomotility, or can be formed outside of the intestine and migrate there via a fistula. In our case, the patient’s enterolith may have formed from the stasis of bile flow in the ileal diverticulum. This case highlights the importance of considering ileal diverticulitis as a broad differential in patients with terminal ileitis seen on imaging after ruling out more common causes.
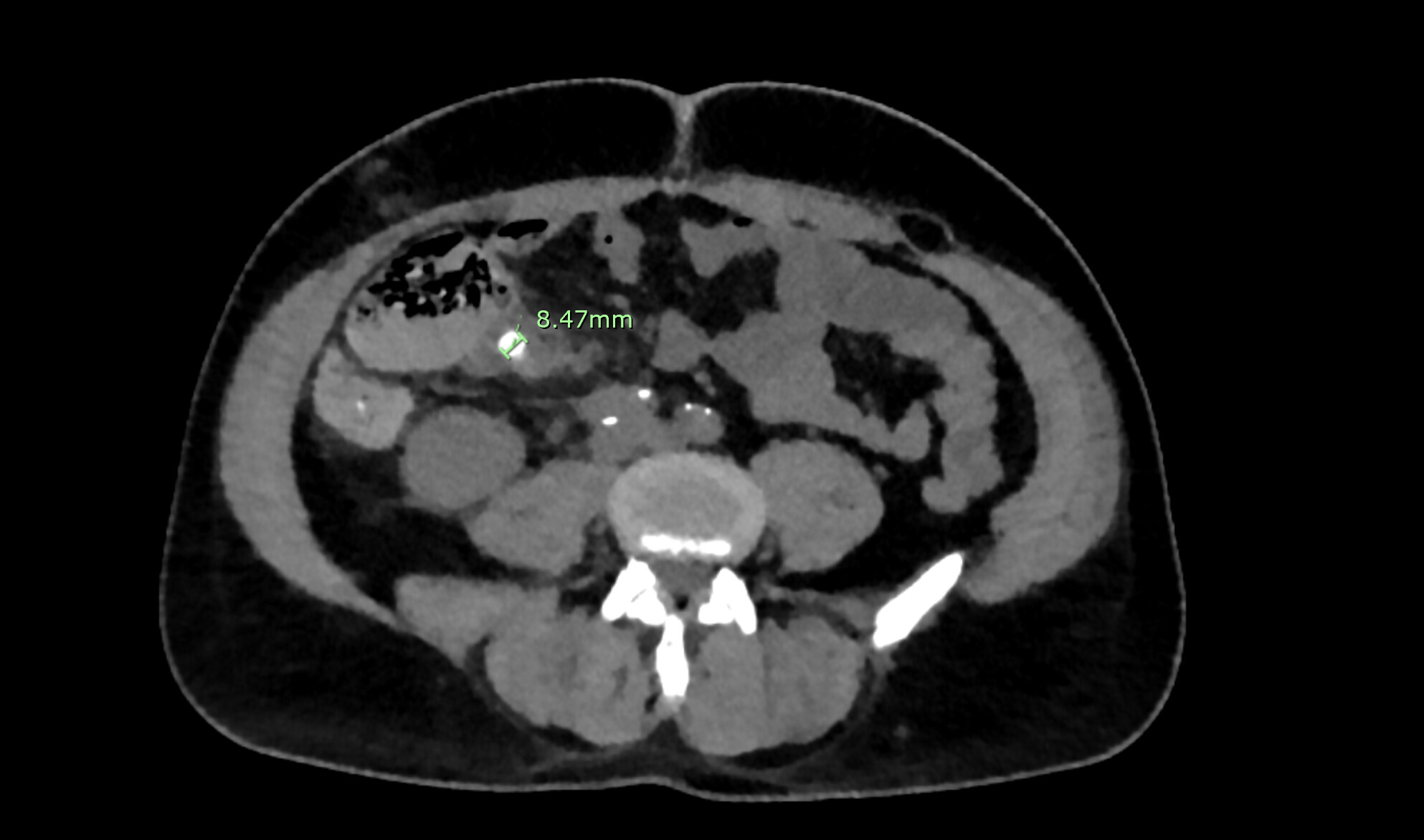
Figure: CT abdomen without contrast demonstrates an 8.47mm enterolith in the terminal ileum.
Disclosures: Christie Polycarpe indicated no relevant financial relationships. Nandakumar Mohan indicated no relevant financial relationships. Oluwanifemi Balogun indicated no relevant financial relationships. Shyam Patel indicated no relevant financial relationships.
Christie Polycarpe, DO, Nandakumar Mohan, DO, Oluwanifemi Balogun, MD, Shyam Patel, MD. P4162 - A Rare Case of Acute Ileal Diverticulitis With Enterolith as a Cause of Isolated Terminal Ileitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.