University of Tennessee Health Science Center Chattanooga, TN
Kristie Liao, DO, Christopher Butler, DO, William Oelsner, MD, Laurie-Anne Swaby, MD University of Tennessee Health Science Center, Chattanooga, TN Introduction: Signet ring cell carcinoma (SRCC) is a rare and aggressive subtype of adenocarcinoma, most commonly originating in the stomach but also found in the colon, breast, bladder, and pancreas. It tends to infiltrate the stomach wall rather than forming a discrete mass, making early detection difficult as patients present with nonspecific symptoms like epigastric pain, nausea, vomiting, and early satiety. SRCC is more common in younger patients and females compared to other gastric cancers. It is also associated with worse prognosis due to early lymphovascular invasion, peritoneal dissemination, and poor response to chemotherapy.
Case Description/
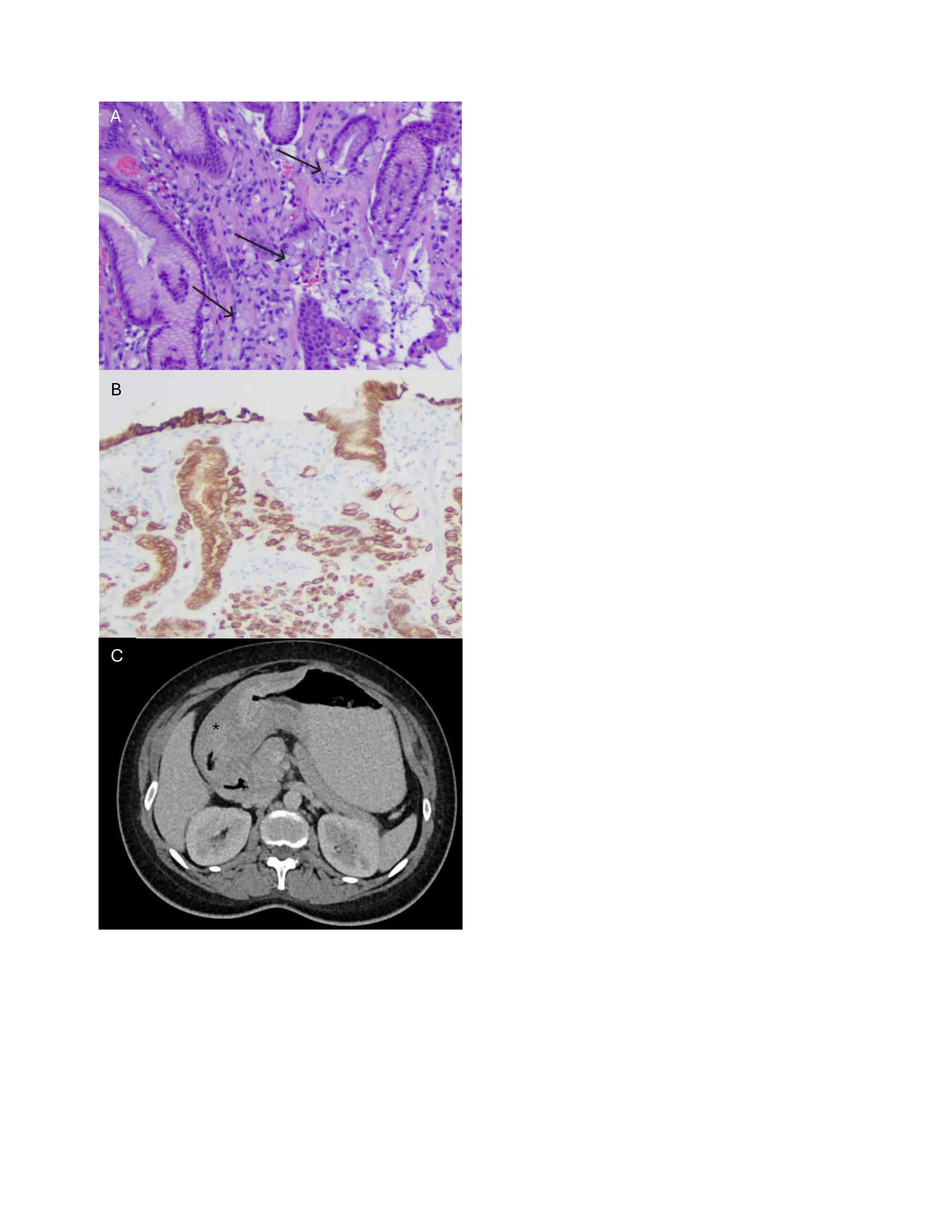
Methods: Our patient is a 31 year old pregnant G5P1031 female with a history of depression, GERD, and nephrolithiasis who presented at 37 weeks gestation with acute on chronic abdominal pain and poor oral intake. She had longstanding epigastric pain, nausea, and vomiting predating her pregnancy, with a delayed EGD due to conception. Imaging revealed distal stomach and proximal duodenal wall thickening concerning for gastroduodenal intussusception. Labs showed elevated liver enzymes, anemia, and thrombocytopenia. Given persistent symptoms and concern for intussusception, she underwent a C section followed by EGD, which showed severe gastric inflammation and mucosal changes concerning for eosinophilic esophagitis (EOE). Biopsies revealed poorly differentiated adenocarcinoma with signet ring cells (Figure A, B) in the gastric antrum and EOE. A staging CT showed mass-like thickening of the gastric antrum (Figure C), pyloric involvement, and enlarged lymph nodes with a dominant mesenteric node measuring 9x14mm. Despite receiving four cycles of FOLFOX, she ultimately required a subtotal gastrectomy, omentectomy, and cholecystectomy. Her course was further complicated by peritoneal carcinomatosis with loculated ascites. Discussion: This rare and challenging diagnosis of SRCC in the setting of pregnancy presents significant diagnostic and therapeutic dilemmas. This aggressive subtype is often diagnosed at an advanced stage due to nonspecific symptoms which could be misattributed to pregnancy. In pregnant patients, imaging and endoscopic evaluation can be further delayed. Management requires a multidisciplinary approach to balance both maternal and fetal health, often requiring an early delivery. Prognosis is typically poor, underscoring the importance of maintaining a high index of suspicion in pregnant patients with persistent gastrointestinal symptoms.
Figure: Figure A: H&E stain of gastric antrum with arrows delineating signet ring cells Figure B: Keratin stain of gastric antrum with evidence of invasive signet ring cell adenocarcinoma Figure C: CT scan with evidence of significant wall thickening of gastric antrum, delineated by asterisk
Disclosures: Kristie Liao indicated no relevant financial relationships. Christopher Butler indicated no relevant financial relationships. William Oelsner indicated no relevant financial relationships. Laurie-Anne Swaby indicated no relevant financial relationships.
Kristie Liao, DO, Christopher Butler, DO, William Oelsner, MD, Laurie-Anne Swaby, MD. P4237 - Signet Ring Adenocarcinoma in Pregnancy: Balancing Maternal and Fetal Health in a Rare Diagnosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.