Bogdan Cristescu, MD, Maria Cristescu, , Tudor Cristescu, , Ana Cristescu, Aurora Healthcare, De Pere, WI Introduction: Emphysematous gastritis is a rare and severe condition cased by gas forming infectious organisms invading the gastric wall and causing intramural gas and gas in the portal venous system. Mortality rate is over 60%. Approximately 75 cases have been reported in the literature. We report a case of emphysematous gastritis treated successfully with conservative management with IV antibiotics, proton pump inhibitors, bowel rest, parenteral nutrition and supportive care.
Case Description/
Methods: A 76-year-old male with past medical history of type 2 diabetes on insulin, prostate cancer presenting with nausea, vomiting with coffee ground emesis and syncope. He was hypotensive on admission and was diagnosed with septic shock with marked leukocytosis with WBC 40,000/mcl, lactic acidosis with lactic acid of 13.8 mmol/L and normal Hb of 14.6 g/dL. CT abdomen and pelvis showed gastric pneumatosis and portal venous gas in the liver, especially in the left main portal vein. EGD revealed a large 15 cm necrotic appearing ulceration in the posterior wall of the stomach involving the gastric body and fundus. Gastric biopsies revealed extensive necrosis and hemorrhage. Patient was intubated in the intensive care unit and placed on pressors, IV fluids, bowel rest, broad- spectrum antibiotics and antifungals. Clinical course was complicated by acute renal failure. Surgical consult recommended conservative management. Patient required parenteral nutrition and clinical condition improved gradually and repeat EGD a week later demonstrating edematous mucosa with superficial ulceration along the posterior wall of the gastric body with a much smaller localized area a necrosis in the gastric fundus on retroflexion approximately 3- 4 cm. The patient was discharged in stable condition and repeat EGD 3 months later revealed complete healing of the gastric mucosa with mild gastritis. Discussion: Emphysematous gastritis requires early recognition by the radiographic appearance of air the gastric wall, which may extend into the portal venous system in a critically ill, septic patient presenting with abdominal pain, nausea, vomiting and possible hematemesis. Diabetes, alcohol abuse and immunosuppression are predisposing factors. Surgical treatment with gastrectomy has been largely replaced by conservative treatment with improved survival.
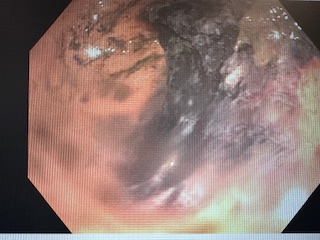
Figure: EGD with large necrotic posterior gastric wall ulceration
Figure: CT abdomen and pelvis with gastric pneumatosis and portal venous gas in the liver
Disclosures: Bogdan Cristescu indicated no relevant financial relationships. Maria Cristescu indicated no relevant financial relationships. Tudor Cristescu indicated no relevant financial relationships. Ana Cristescu indicated no relevant financial relationships.
Bogdan Cristescu, MD, Maria Cristescu, , Tudor Cristescu, , Ana Cristescu, . P4231 - Emphysematous Gastritis: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.