P4219 - Synchronous Diffuse Large B-Cell Lymphoma and Gastric Adenocarcinoma: A Rare Dual Malignancy Presenting With Gastric Outlet Obstruction and Fistulous Complication
Idan Grossmann, MD1, Aubin Attila, MD2, Harshavardhan Sanekommu, MD2, Vera Hapshy, DO3, Natasha Campbell, MD2, Lee Peng, MD, PhD2, Angelo Chinnici, MD2, Mohammad Hossain, MD2 1Hackensack Meridian Health, Bradley Beach, NJ; 2Hackensack Meridian Health, Neptune, NJ; 3Hackensack Meridian JSUMC, Neptune City, NJ Introduction: Concurrent presentation of two primary gastrointestinal (GI) cancers is extremely rare, with limited cases reported in the literature. Primary gastrointestinal lymphoma comprises less than 5% of GI malignancies, while gastric adenocarcinoma remains one of the most prevalent GI cancers globally. The synchronous occurrence of diffuse large B-cell lymphoma (DLBCL) and gastric adenocarcinoma presents unique diagnostic and therapeutic challenges. This case highlights a rare instance of concurrent dual GI malignancies complicated by obstruction and fistulization, requiring complex multidisciplinary management.
Case Description/
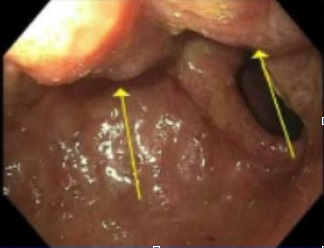
Methods: A 69-year-old male with a past medical history of inguinal hernia repair presented with one week of intractable nausea and vomiting. Two months earlier, he had reported abdominal discomfort, distention, anorexia, and a 15-pound weight loss over four weeks. CT imaging showed mural thickening of the duodenum, colonic thickening, and a fistula between the duodenum and ascending colon. EGD revealed a 4 cm cratered gastric ulcer and a large fungating duodenal mass. Biopsies confirmed T3N2 poorly differentiated gastric adenocarcinoma with signet ring cells and DLBCL involving the duodenum with colonic fistula.
On admission, he was afebrile and hemodynamically stable, with mild abdominal tenderness. Laboratory studies showed leukocytosis, anemia, and elevated alkaline phosphatase. A port was placed, and R-CHOP chemotherapy was initiated for lymphoma. He developed bilateral segmental pulmonary emboli requiring anticoagulation. Shortly thereafter, he acutely decompensated with respiratory failure and was found to have a bowel perforation. He underwent emergent surgery, including right colectomy, partial Whipple, and gastrectomy. His course was complicated by ongoing sepsis, transfusion requirements, and multiorgan failure. Despite further surgical interventions, he remained critically ill and passed away. Discussion: Synchronous primary gastrointestinal malignancies are exceedingly rare and require highly individualized treatment strategies. The initial plan to treat lymphoma first with chemotherapy was derailed by perforation, necessitating emergent surgery. This illustrates the challenges in managing coexisting cancers, where treatment of one malignancy may exacerbate complications of the other. Given the rarity of such presentations, additional case reports are essential to guide management strategies and inform clinical decision-making in similarly complex scenarios.
Disclosures: Idan Grossmann indicated no relevant financial relationships. Aubin Attila indicated no relevant financial relationships. Harshavardhan Sanekommu indicated no relevant financial relationships. Vera Hapshy indicated no relevant financial relationships. Natasha Campbell indicated no relevant financial relationships. Lee Peng indicated no relevant financial relationships. Angelo Chinnici indicated no relevant financial relationships. Mohammad Hossain indicated no relevant financial relationships.
Idan Grossmann, MD1, Aubin Attila, MD2, Harshavardhan Sanekommu, MD2, Vera Hapshy, DO3, Natasha Campbell, MD2, Lee Peng, MD, PhD2, Angelo Chinnici, MD2, Mohammad Hossain, MD2. P4219 - Synchronous Diffuse Large B-Cell Lymphoma and Gastric Adenocarcinoma: A Rare Dual Malignancy Presenting With Gastric Outlet Obstruction and Fistulous Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.