Nupur Savalia, MD, Faizi Hai, MD, Sevag Hamamah, DO Scripps Mercy Hospital, San Diego, CA Introduction: Gastric outlet obstruction (GOO) is the intrinsic or extrinsic mechanical blockage of gastric emptying, generally at the distal stomach or duodenum arising from various benign or malignant conditions. Typical symptoms of GOO are nonspecific. The most common causes of GOO are generally benign conditions including gastric and duodenal ulcers. Malignant causes of GOO typically include cancers arising from the stomach, duodenum, pancreas, biliary tree, and liver, and very rarely from metastases. We present the case of GOO induced by metastases in the setting of breast cancer recurrence.
Case Description/
Methods: A 64 year old female with past medical history of left breast cancer in remission for 2 years (not on treatment) who presented with a 3 day history of nausea, nonbilious vomiting, and reflux symptoms. She also reported a 1 month history of intermittent gnawing epigastric pain at night. CT abdomen pelvis revealed gastric and proximal duodenal distention with notable transition point in the second portion of duodenum consistent with GOO. Gastroenterology performed endoscopic evaluation which revealed a large volume of retained food in the gastric body. A regular endoscope was unable to pass into the duodenum so an ultra slim endoscope was trialed which eventually passed through with difficulty. No mass was appreciated in this area, but the tissue was noted to be very edematous. Duodenal biopsy did not show any significant histopathologic findings. General surgery was consulted and proceeded with an exploratory laparotomy and roux-en-y gastrojejunostomy. Histopathology from the surgical biopsy of the omentum revealed metastatic carcinoma consistent with breast origin. Discussion: This case demonstrates the importance of postulating a broad set of differentials for GOO, including both non-malignant and malignant causes. Although breast cancer is the most common cancer diagnosis in women, peritoneal and gastrointestinal metastases are rare, making GOO secondary to breast carcinoma a challenging diagnosis. Clinicians must consider this diagnosis even in cases where breast cancers have been in remission for a long time alongside more common causes of GOO such as pancreatic and gastric carcinomas and peptic ulcer disease. Treatment for GOO due to malignancy depends upon the underlying cause but typical options include endoscopic or surgical gastrojejunostomy or placement of an enteral stent.
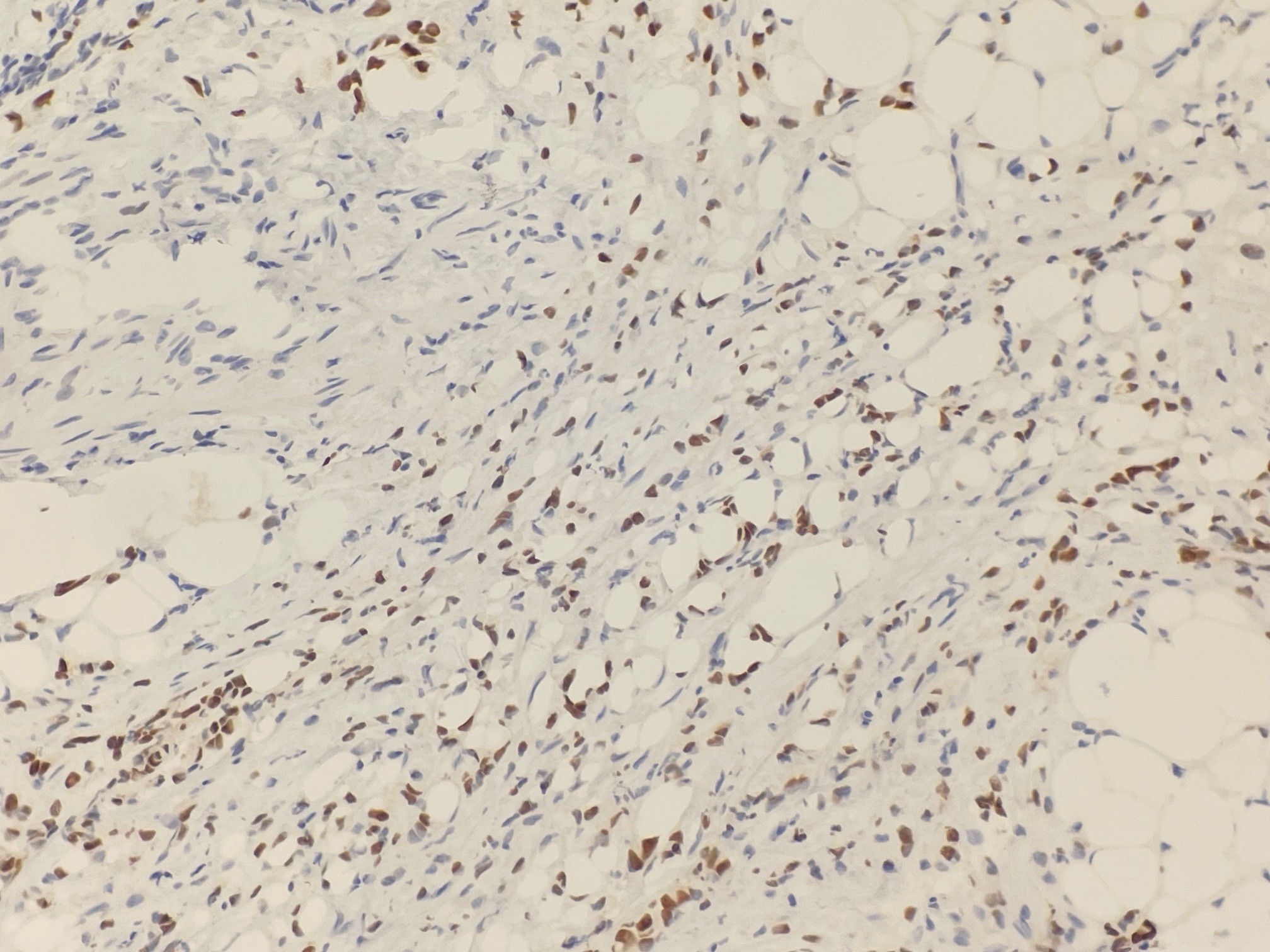
Figure: Histological image with positive GATA-binding protein 3 (GATA3) stain consistent with metastatic carcinoma of breast origin
Figure: CT abdomen and pelvis with prominent distention of the stomach and proximal duodenum with transition at the second portion of the duodenum without discrete mass
Disclosures: Nupur Savalia indicated no relevant financial relationships. Faizi Hai indicated no relevant financial relationships. Sevag Hamamah indicated no relevant financial relationships.
Nupur Savalia, MD, Faizi Hai, MD, Sevag Hamamah, DO. P4278 - Breast Cancer Recurrence Presenting as Gastric Outlet Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.