P4269 - Gastric Outlet Obstruction Secondary to Gastric Duplication Cyst With Pancreatobiliary Adenocarcinoma Arising From Ectopic Pancreatic Tissue: A Follow-Up Case From ACG 2024
Elmhurst Hospital Center / Icahn School of Medicine at Mount Sinai Queens, NY
Bibhuti Adhikari, MD, Woo Suk Kim, DO, Krishna Gurram, MD, Tasur Seen, MD Elmhurst Hospital Center / Icahn School of Medicine at Mount Sinai, Queens, NY Introduction: Gastrointestinal tract duplications (GTDs) are rare congenital anomalies that can occur anywhere along the alimentary tract, most commonly in the ileum. Gastric duplication cysts (GDCs) account for < 10% of all GTDs and may remain asymptomatic or present with bleeding, infection, or gastric outlet obstruction (GOO). Malignant transformation is rare but possible, particularly with ectopic tissue. We present a follow up case of GDC causing GOO (previously submitted at ACG 2024), which was ultimately diagnosed as pancreatobiliary adenocarcinoma arising from ectopic pancreatic tissue.
Case Description/
Methods: A 65-year-old man with no significant history presented with abdominal pain, postprandial nausea, non-bloody vomiting, dysphagia, and weight loss. He had not had a bowel movement for 6 days. Exams showed tachycardia and hypotension; labs revealed hypokalemic, hypochloremic metabolic alkalosis. CT abdomen showed a distended stomach and a 6 cm multiloculated cystic mass in the gastric antrum. NG tube drainage relieved symptoms. EGD revealed two 20 mm submucosal cystic papules at the pylorus; EUS with FNA showed multiple non-communicating cysts in the pylorus, duodenal bulb, and deep gastric wall, suggestive of duplication cysts. Cyst fluid CEA was elevated (709 ng/mL), and repeat aspiration with stent placement was performed due to persistent obstruction. Pathology revealed moderately differentiated adenocarcinoma with pancreatobiliary features arising from ectopic pancreatic tissue within the GDC. MRI pancreas was negative for primary disease. Ultimately, the patient underwent robotic distal gastrectomy with Billroth II. Multidisciplinary tumor board recommended modified FOLFIRINOX; the patient completed 9 cycles with no recurrence on PET/CT. Discussion: GDCs are rare and can mimic pancreatic neoplasms when they contain ectopic pancreatic tissue. Malignant transformation, while uncommon, may occur via oncofetal antigen expression or ectopic tissue dysplasia. Our case met criteria for carcinoma arising from ectopic pancreas, confirmed by histology and immunoprofile (CA19-9+, CK7+, CEA+, CK20+, TTF1+, CDX2+). This case emphasizes the importance of recognizing GDCs, evaluating cystic lesions carefully, and considering malignancy in atypical presentations of GOO.
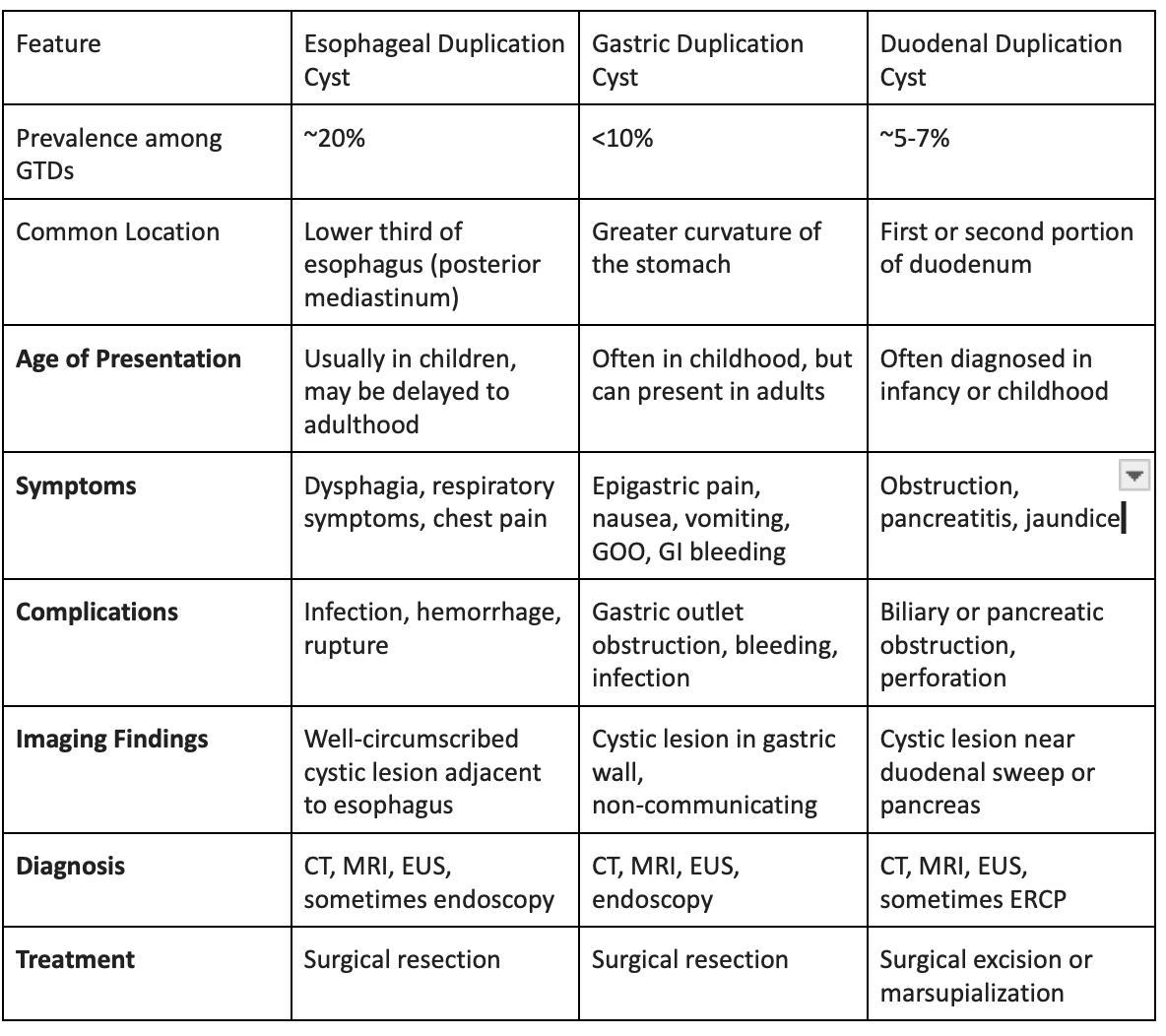
Figure: Comparative Table: Esophageal vs. Gastric vs. Duodenal Duplication Cysts
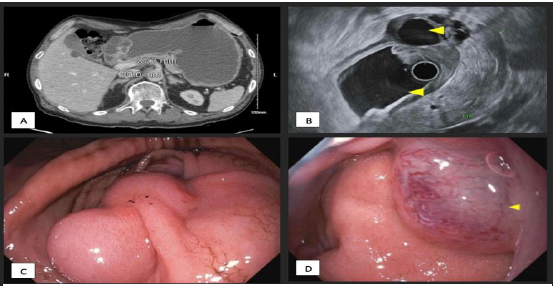
Figure: Figure A: CTAP demonstrating multiloculated cystic mass in gastric antrum; B: EUS findings; C:Bilobed cystic mass in pre-pylorus stomach; D: Cystic mass in the duodenum
Disclosures: Bibhuti Adhikari indicated no relevant financial relationships. Woo Suk Kim indicated no relevant financial relationships. Krishna Gurram indicated no relevant financial relationships. Tasur Seen indicated no relevant financial relationships.
Bibhuti Adhikari, MD, Woo Suk Kim, DO, Krishna Gurram, MD, Tasur Seen, MD. P4269 - Gastric Outlet Obstruction Secondary to Gastric Duplication Cyst With Pancreatobiliary Adenocarcinoma Arising From Ectopic Pancreatic Tissue: A Follow-Up Case From ACG 2024, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.