Prisma Health, University of South Carolina School of Medicine Columbia, SC
Susan Feldman, MD1, Nelson Gonzales, BS2, Simran Joshi, MD3, Devendra Enjamuri, MD1 1Prisma Health, University of South Carolina School of Medicine, Columbia, SC; 2University of South Carolina School of Medicine, Columbia, SC; 3Yale New Haven Health, Bridgeport Hospital, Bridgeport, CT Introduction: Gastric neuroendocrine carcinomas (NECs) are rare, high-grade malignancies accounting for less than 1% of all gastric neoplasms. They are classified into small and large cell types, the latter being exceedingly uncommon and typically pulmonary in origin. Gastric large cell neuroendocrine carcinoma (LCNEC) is aggressive, often diagnosed at an advanced stage, and carries a poor prognosis due to rapid progression and limited treatment options. Early detection via endoscopic surveillance is rare, as patients are usually asymptomatic or present with nonspecific gastrointestinal symptoms. We present a rare case of incidentally discovered gastric LCNEC in a gastric polyp.
Case Description/
Methods: A 74-year-old female with a past medical history of COPD, hypertension, OSA, and CKD3 presented with new-onset dysphagia and concern for food impaction. EGD did not reveal an obstructive lesion but identified a solitary gastric polyp in the proximal gastric body. Biopsy of the lesion was initially reported as poorly differentiated adenocarcinoma. A repeat EGD with ESD was performed, revealing a medium sized polypoid mass within the gastric body. Due to extensive fibrosis and a full-thickness defect during resection, the tumor was removed in two segments. Histopathologic analysis identified large cell neuroendocrine carcinoma, measuring 1.5 cm in greatest dimension. A subsequent PET scan showed no evidence of metastatic disease. The patient was referred to medical oncology and initiated on platinum-based chemotherapy with etoposide (VP-16) and cisplatin. Discussion: Gastric large cell neuroendocrine carcinoma (LCNEC) is a rare and aggressive malignancy with few reported cases. Its endoscopic appearance can mimic adenocarcinoma or benign polyps, posing a diagnostic challenge. In this case, initial superficial biopsies suggested poorly differentiated adenocarcinoma, but the actual diagnosis was only established after endoscopic submucosal dissection enabled deeper sampling. This underscores the limitations of superficial biopsies, particularly for submucosal or high-grade lesions. Given the tumor’s aggressive nature and submucosal invasion, timely systemic staging and oncologic intervention are essential. This case also highlights the importance of biopsying atypical-appearing gastric polyps and the diagnostic value of deeper resection in identifying rare but serious pathologies.
Figure: initial EGD of gastric polyp, pathology reported as poorly differentiated adenocarcinoma
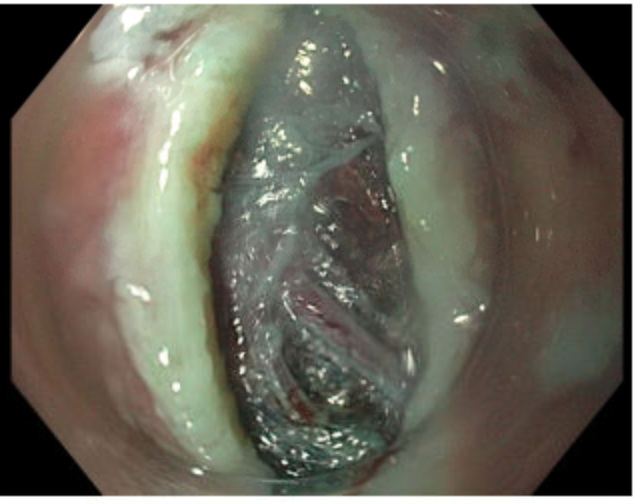
Figure: submucosal fibrosis on dissection, pathology from biopsy with LCNEC
Disclosures: Susan Feldman indicated no relevant financial relationships. Nelson Gonzales indicated no relevant financial relationships. Simran Joshi indicated no relevant financial relationships. Devendra Enjamuri indicated no relevant financial relationships.
Susan Feldman, MD1, Nelson Gonzales, BS2, Simran Joshi, MD3, Devendra Enjamuri, MD1. P4268 - An Unusual Gastric Polyp: A Rare Case of Large Cell Neuroendocrine Carcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")