University of Utah School of Medicine Salt Lake City, UT
Benjamin Gow-Lee, MD1, Mina Awadallah, MD, MSc2, Jessica Schmitt, MD1, John Erikson Yap, MD, MBA, FACG3 1University of Utah School of Medicine, Salt Lake City, UT; 2University of Utah, Salt Lake City, UT; 3University of Utah Health, Salt Lake City, UT Introduction: Gastric polyps are commonly seen on diagnostic endoscopies. The most common types of polyps are fundic gland and hyperplastic polyps. Oxyntic gland adenomas (OGAs) are rare, benign epithelial neoplasms arising from the gastric body or fundus. We present one such case.
Case Description/
Methods: A 42-year-old woman with a history of type 2 diabetes and RYGB presented with chronic, intermittent postprandial epigastric pain. She denied taking any NSAIDs, Her physical exam and was unremarkable with normal vital signs. Initial laboratory work-up came back with normal complete blood count and comprehensive metabolic panel. A Helicobacter pylori stool antigen was negative. Upper endoscopy was pursued and demonstrated intact Roux-en-Y anatomy with a 5 cm gastric pouch and a dilated gastrojejunal anastomosis measuring approximately 20–25 mm. The jejunal limbs appeared normal. A small sessile gastric polyp (Figure 1) was identified and resected using a cold snare. Random biopsies from the gastric pouch and small bowel came back normal, with no evidence of infection. Histopathology confirmed the gastric polp as an oxyntic gland adenoma. The patient was started on omeprazole and subsequently reported improvement in her postprandial symptoms. Discussion: OGAs are rare, benign epithelial neoplasms arising from oxyntic mucosa. They are predominantly found in the gastric body and fundus. If found to be invading the submucosa, it is classified as gastric adenocarcinoma of fundic gland type (GA-FG). Neither OGA or GA-FG are associated with H. pylori infection. OGA and GA-FG tend to grow slowly and only rarely invade lymphatic or vascular systems. There are no reports of mortality from OGA or GA-FG. Due to their rarity, there are no guidelines for treatment, but typically endoscopic resection are suitable initial treatments for both OGA and GA-FG. Given their rarity, further data are needed to clarify the clinical implications and guide management of oxyntic gland adenomas.
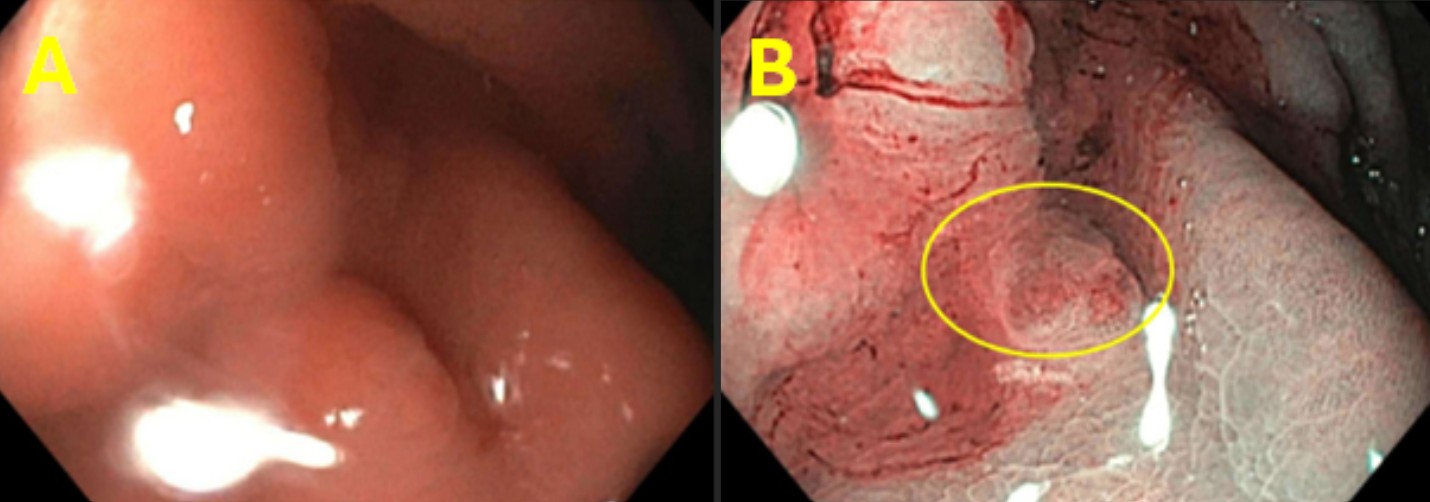
Figure: Sessile polyp found to be oxyntic gland adenoma on (A) white light and (B) Narrow Band Imaging.
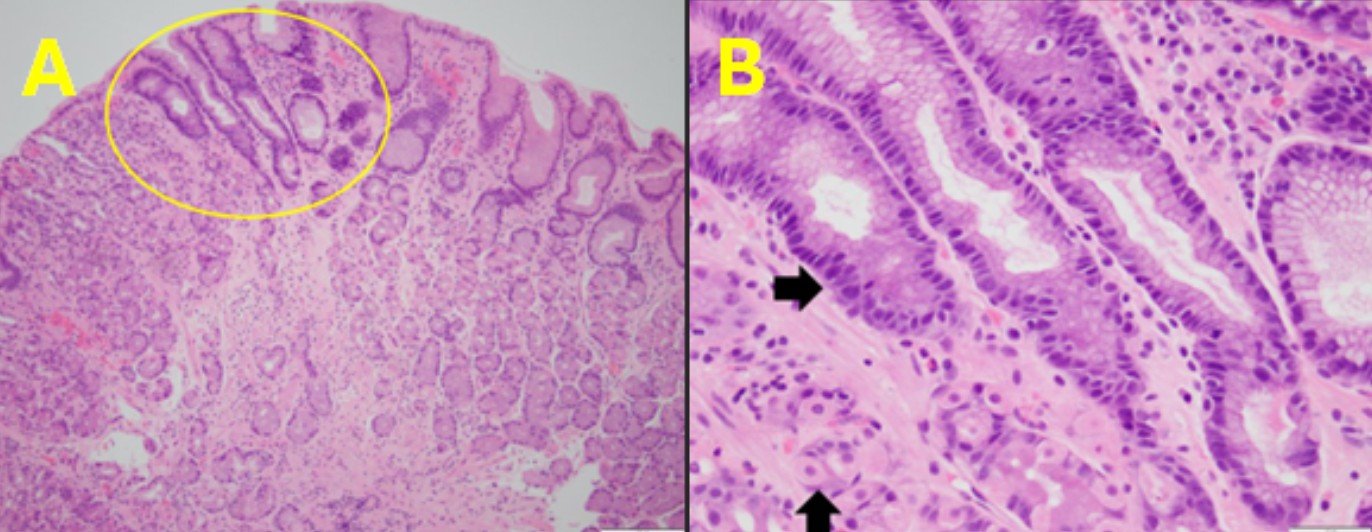
Figure: Hematoxylin and Eosin (H&E) stain demonstrating a (A) low-power view of the gastric oxyntic mucosa with a well-circumscribed (encircled) focus of mildly increased glandular crowding. Image was captured with a 10x objective. (B) Demonstrates a high-power view of the gastric oxyntic mucosa (up arrow pointing out normal parietal cells along mucus cells) with oxyntic epithelial cells with mild nuclear enlargement (right arrow). Image was captured with a 40x objective.
Disclosures: Benjamin Gow-Lee indicated no relevant financial relationships. Mina Awadallah indicated no relevant financial relationships. Jessica Schmitt indicated no relevant financial relationships. John Erikson Yap: Phathom Pharmaceutical – Speakers Bureau. Steris – Consultant.
Benjamin Gow-Lee, MD1, Mina Awadallah, MD, MSc2, Jessica Schmitt, MD1, John Erikson Yap, MD, MBA, FACG3. P4266 - A Rare Gastric Polyp, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Benjamin Gow-Lee, MD (he/him/his) photo")