Joanna Lenik, MD1, Gulce Karaca, MD2, Jennifer Harley, MD3, David Frank, MD3 1New York Medical College/Metropolitan Hospital Center, New York, NJ; 2NYC Health + Hospitals/Woodhull, Brooklyn, NY; 3NYC Health + Hospitals/Metropolitan, New York, NY Introduction: Acute gastric necrosis is a rare but serious complication of massive gastric distension. The stomach’s rich vascular supply generally protects it from ischemia; however, extreme distension can compromise perfusion, leading to transmural necrosis. Psychiatric illnesses such as schizophrenia and antisocial personality disorder may increase the risk of atypical gastrointestinal presentations due to altered behavior, poor symptom reporting, or medication side effects.
Case Description/
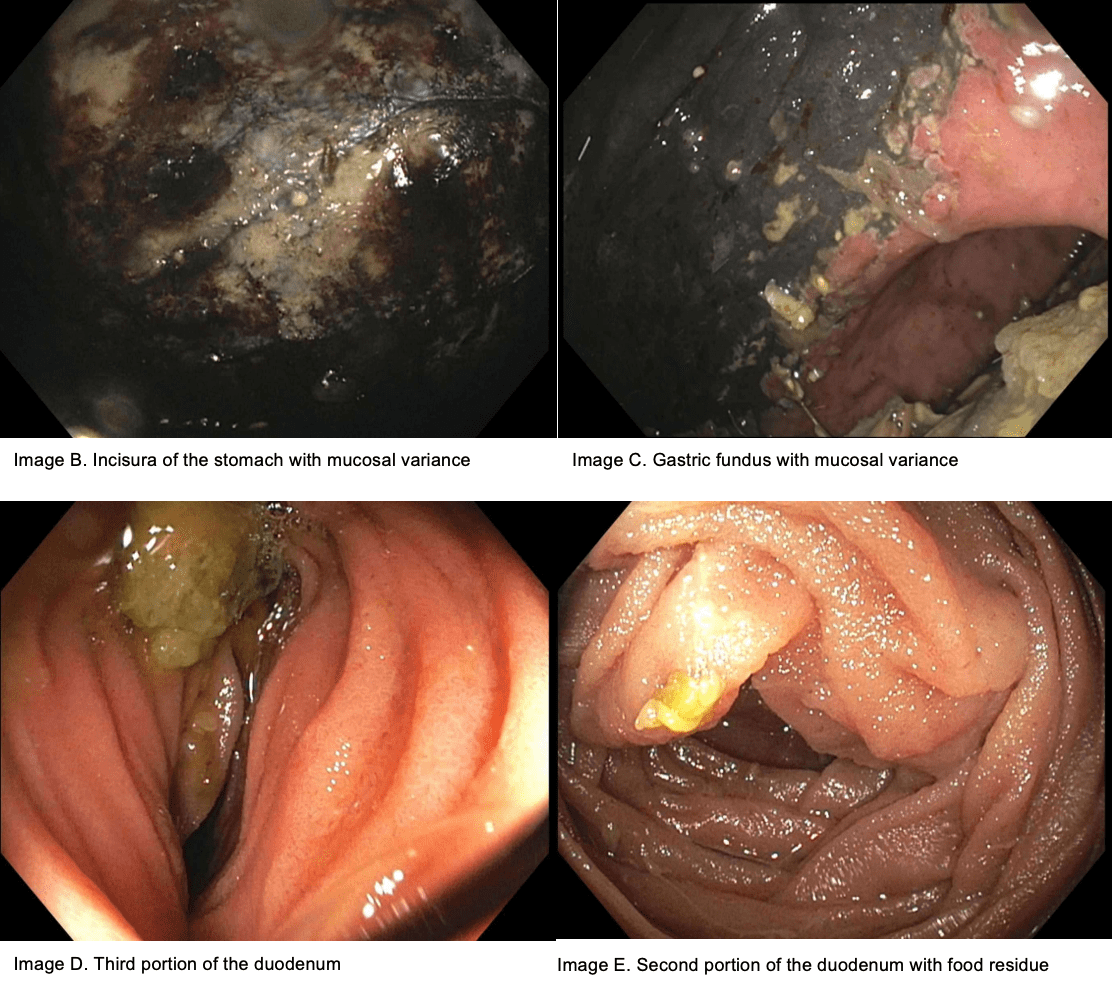
Methods: We report the case of a 46-year-old male with a known history of schizophrenia and antisocial personality disorder who presented with a 24-hour history of progressive abdominal pain and intractable vomiting. On admission, the patient experienced rapid clinical deterioration with respiratory failure requiring emergent intubation. Physical examination revealed significant abdominal distension and tenderness. A nasogastric tube was placed, yielding approximately 6 liters of dark, non-feculent gastric fluid. CT imaging of the abdomen showed a massively distended stomach exerting extrinsic compression on the duodenum, raising suspicion for a gastric outlet obstruction. No intraluminal masses, volvulus, or strictures were identified. Subsequent esophagogastroduodenoscopy (EGD) revealed diffuse necrosis of the gastric wall, sparing the antrum, without evidence of an obstructive lesion or foreign body. Discussion: The etiology of the severe gastric distension and necrosis in this patient remains unclear. Proposed mechanisms include acute gastric dilatation (AGD), possibly linked to disordered eating or impaired gastric motility secondary to psychiatric illness or medication side effects. Other considerations include functional gastric outlet obstruction due to stomach compression of the duodenum, delayed gastric emptying, or subclinical episodes of gastric volvulus. The absence of a mechanical obstruction and the sparing of the antrum are unusual findings that add complexity to the case. This report emphasizes the need for high clinical suspicion and rapid intervention in patients presenting with gastric distension, especially those with psychiatric comorbidities that may delay diagnosis.
Figure: CT scan of the abdomen
Figure: Endoscopy findings
Disclosures: Joanna Lenik indicated no relevant financial relationships. Gulce Karaca indicated no relevant financial relationships. Jennifer Harley indicated no relevant financial relationships. David Frank indicated no relevant financial relationships.
Joanna Lenik, MD1, Gulce Karaca, MD2, Jennifer Harley, MD3, David Frank, MD3. P4262 - From Balloon to Blackout - Acute Gastric Necrosis in a Patient With Severe Gastric Distension: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.