Nisar Amin, MD, Mai T. Tran, MD, Ebubekir Daglilar, MD, Harleen Chela, MD Charleston Area Medical Center, Charleston, WV Introduction: Kaposi sarcoma (KS), a malignancy linked to HHV-8, is the most common neoplasm in HIV patients. While it typically presents with skin lesions, visceral involvement occurs in up to 25% of cases. We present a case of KS with gastric and duodenal involvement confirmed by endoscopy and biopsy.
Case Description/
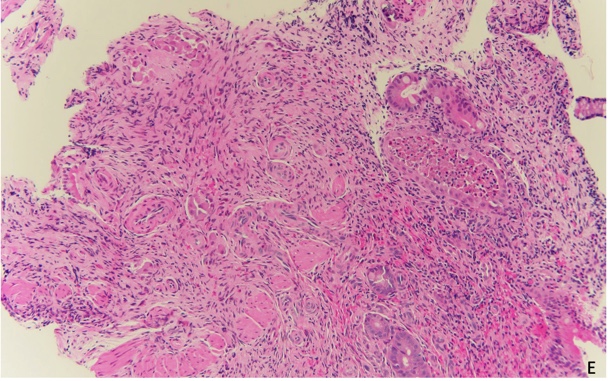
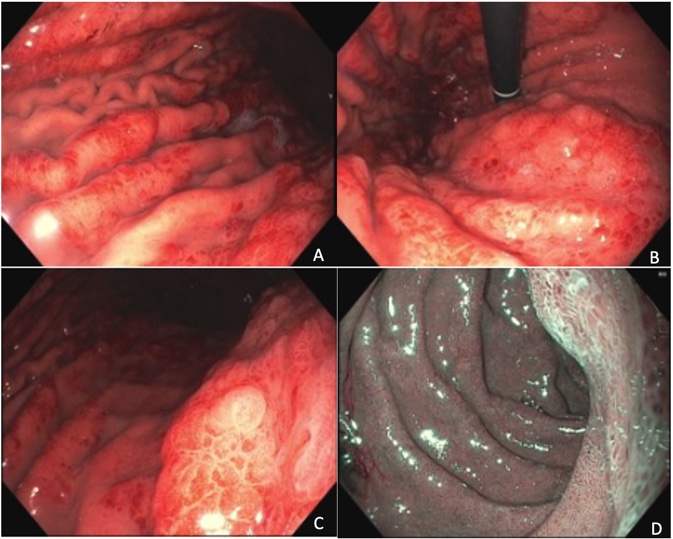
Methods: A 35-year-old male with a history of HIV on HAART (latest viral load undetectable; CD4 count 47) pulmonary nodules and cutaneous lesions consistent with Kaposi sarcoma (KS) referred to GI for iron deficiency anemia evaluation. He denied melena, hematochezia, hematemesis, abdominal pain, or significant weight loss. He reported chronic GERD symptoms, nausea, vomiting, and diarrhea. Upper and lower endoscopy were performed to evaluate for potential gastrointestinal sources of IDA. The colonoscopy was unremarkable. Esophagogastroduodenoscopy (EGD) revealed diffuse erythema and thickened gastric folds with spontaneous oozing throughout the fundus, cardia, and body (Figures A, B and C). Several 1 cm polypoid lesions were noted in the antrum. Subtle areas of erythema were observed in the second and third portions of the duodenum (Figure D). Biopsies were taken from these areas. Histopathology confirmed Kaposi sarcoma in the gastric pylorus (Figure E) and duodenum, with probable early involvement of the antrum. Immunohistochemistry was positive for CD31 and negative for CD117 and DOG1, ruling out GIST. H. pylori testing was negative; Ki-67 index was 1%. The patient was treated with doxorubicin at 20 mg/m² for 9 months. Follow-up endoscopy showed resolution of duodenal and gastric involvement. Clinically, the patient showed improvement in skin lesions. His CD4 count remained below 200, and he continues on HAART. Discussion: Gastrointestinal Kaposi sarcoma (KS) can occur in HIV patients independently of cutaneous involvement. These lesions may be asymptomatic or present with a range of symptoms, from mild nausea and vomiting to more severe manifestations such as hemorrhage, abdominal pain, gastric outlet obstruction, or intussusception. Endoscopically, gastrointestinal Kaposi sarcoma (KS) can present as erythematous, maculopapular, or polypoid lesions. These lesions are typically submucosal, which can make histopathological diagnosis difficult . Immunostaining for CD31, CD34, and LNA-1 helps in diagnosing GI Kaposi sarcoma. Currently, routine endoscopy isn’t recommended for all KS patients but may be appropriate in select cases.
Figure: Figures A, B, C: Diffuse erythema and thickened gastric folds with spontaneous oozing throughout the fundus, cardia, and body. Figure D: Subtle areas of erythema in the second and third portions of the duodenum, depicted under NBI.
Figure: Fragment of gastric mucosa with lesion in the lamina propria composed of spindle cells proliferation with moderate atypia and arranged in vague fascicle. Fascicles separated by slit-like spaces filled with erythrocytes. (H&E, 20X).
Disclosures: Nisar Amin indicated no relevant financial relationships. Mai Tran indicated no relevant financial relationships. Ebubekir Daglilar indicated no relevant financial relationships. Harleen Chela indicated no relevant financial relationships.
Nisar Amin, MD, Mai T. Tran, MD, Ebubekir Daglilar, MD, Harleen Chela, MD. P4240 - Gastrointestinal Involvement of Kaposi Sarcoma: A Case Report of Gastric and Duodenal Lesions, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.