Muhammad Sohaib Alvi, MBBS, MD1, Furqan Ahmed, MD1, Mohamed A. Ebrahim, MD1, George Atia, MD1, Mohamed Boshnaf, MD, MPH2, Yasmin Gerais, MBBS, MD3, Ashok Kumar, MD1, Alizay Khan, MD1, Sunny Kumar, MD4 1Ascension Saint Joseph Hospital, Chicago, IL; 2Prime Health SJMC, Lockport, IL; 3Saint Joseph medical center, Plainfield, IL; 4Wright Center for Graduate Medical Education, Scranton, PA Introduction: Emphysematous gastritis (EG) is a rare, potentially fatal infection of the gastric wall caused by gas-forming organisms. Portal venous gas (PVG), when present, is typically associated with intestinal ischemia and often prompts urgent surgical intervention. However, in certain cases, imaging severity may not correlate with clinical presentation. We report a rare case of EG with extensive PVG that was managed conservatively in a hemodynamically stable patient.
Case Description/
Methods: A 65-year-old woman with hypertension, type 2 diabetes, stage 3B chronic kidney disease, COPD, and opioid use disorder (on methadone maintenance) presented with two days of right-sided abdominal pain and diarrhea. On admission, she was afebrile and hemodynamically stable. Labs showed WBC 12.3 x10⁹/L, creatinine 4.81 mg/dL (baseline ~1.4), and lactate 1.3 mmol/L. Non-contrast CT revealed gastric pneumatosis and extensive PVG—typically associated with gastric ischemia or sepsis. Despite these findings, the patient had no peritoneal signs or systemic toxicity. She received intravenous fluids, electrolyte replacement, and empiric piperacillin-tazobactam. Blood cultures, Clostridioides difficile testing, and a GI pathogen panel were negative. General Surgery recommended conservative management. EGD showed a 1.5 cm non-bleeding gastric ulcer and ischemic changes seen as purplish colored mucosa in the body with erythema and ulceration; Helicobacter pylori via biopsy testing was negative. Colonoscopy revealed incidental tubular adenomas and diverticulosis. Her abdominal symptoms and renal function improved over a five-day period. She was discharged on oral antibiotics and a proton pump inhibitor, with outpatient endoscopic follow-up planned. Discussion: This case shows that EG with PVG may not require surgery when patients are clinically stable. Most reported cases involve surgical or ICU-level care, but our patient recovered fully with conservative therapy. Despite radiologic severity, clinical context remains paramount in guiding intervention. Methadone-related dysmotility may have predisposed to mucosal injury and secondary infection, though causality remains unclear. The patient remained clinically well at discharge, with outpatient endoscopic reassessment scheduled. This case underscores the expanding role of non-operative management in clinically stable patients with severe-appearing EG.
Formatting support was provided using a generative AI tool under author supervision, in accordance with ACG guidelines.
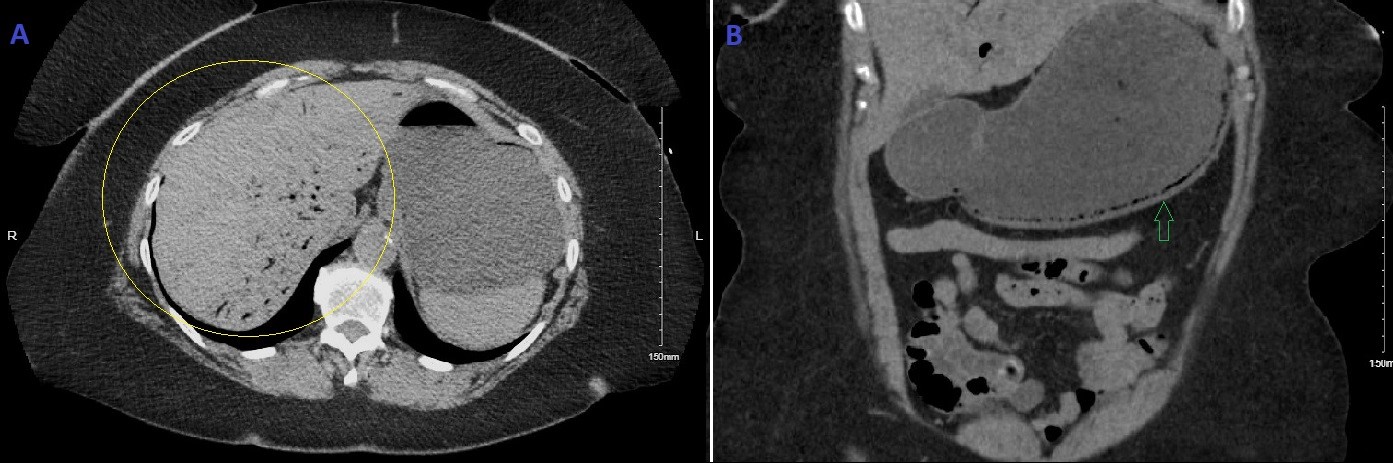
Figure: Figure A: Axial CT showing extensive portal venous gas (branching lucencies) in the liver. (Yellow circle) Figure B: Coronal CT showing intramural gas in the gastric wall, consistent with emphysematous gastritis. (Green arrow)
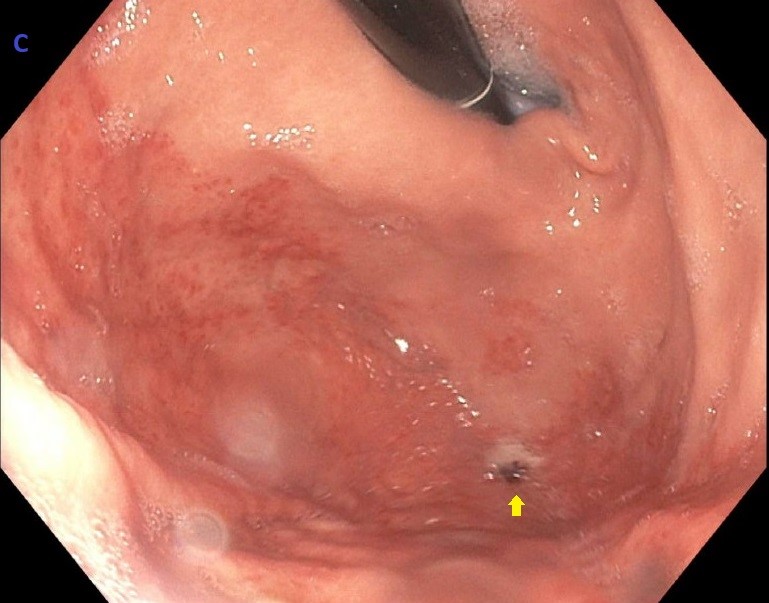
Figure: Figure C: EGD showing 1.5 cm non-bleeding gastric ulcer (Yellow arrow) and surrounding ischemic changes seen as purplish colored mucosa in the body with erythema and ulceration
Disclosures: Muhammad Sohaib Alvi indicated no relevant financial relationships. Furqan Ahmed indicated no relevant financial relationships. Mohamed Ebrahim indicated no relevant financial relationships. George Atia indicated no relevant financial relationships. Mohamed Boshnaf indicated no relevant financial relationships. Yasmin Gerais indicated no relevant financial relationships. Ashok Kumar indicated no relevant financial relationships. Alizay Khan indicated no relevant financial relationships. Sunny Kumar indicated no relevant financial relationships.
Muhammad Sohaib Alvi, MBBS, MD1, Furqan Ahmed, MD1, Mohamed A. Ebrahim, MD1, George Atia, MD1, Mohamed Boshnaf, MD, MPH2, Yasmin Gerais, MBBS, MD3, Ashok Kumar, MD1, Alizay Khan, MD1, Sunny Kumar, MD4. P4216 - Emphysematous Gastritis With Portal Venous Gas: A Case for Conservative Management in a Clinically Stable Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")