Jeevin Singh Sandhu, DO1, Sneha Kannan, BS2, Antony Mathew, MD3, Kyle Schneider, MD1, Parvez Mantry, MD, CPE1 1Methodist Dallas Medical Center, Dallas, TX; 2Kansas City University, Kansas City, MO; 3Methodist Dallas Medical Center, Irving, TX Introduction: Duodenal diverticula are typically silent and are found incidentally, however in rare cases they can lead to small bowel obstruction (SBO). While most SBOs stem from adhesions or scarring, food impaction is an uncommon cause, especially in the small intestine. This case highlights a rare instance where a single impacted whole curry leaf led to a partial small bowel obstruction.
Case Description/
Methods: A 78-year-old male presented to our clinic for ongoing management of GERD, colon polyps, Barrett’s esophagus, and pancreatitis. He had recently been evaluated at an outside hospital (OSH) for persistent nausea in the setting of prostate cancer, for which he had completed radiation therapy a few months earlier. At that time, a small bowel series showed dilation of the small bowel up to 3.8 cm with no complete obstruction. CT imaging revealed numerous duodenal diverticula, diffuse small bowel dilation, wall thickening, and mesenteric edema. Lab work showed a mildly elevated white blood cell count.
During a follow-up telemedicine visit, the patient reported feeling well. It was then decided to proceed with endoscopic evaluation. Esophagogastroduodenoscopy (EGD) revealed normal findings in the esophagus and stomach, but food residue was noted in the third portion of the duodenum. Upon inspection, that residue was determined to be an entire impacted curry leaf. Video capsule endoscopy later confirmed the presence of diverticula distally to the impaction. It was suspected that the curry leaf was the etiology of the patient’s partial small bowel obstruction. The leaf was removed, and the patient was advised to resume his prior diet and follow up in 4 to 6 weeks. Discussion: Duodenal diverticula are usually asymptomatic and rarely require intervention. However, food impaction can lead to complications such as small bowel obstruction or diverticulitis. In this case, an impacted curry leaf was found to be the likely cause of our patient’s resulting obstruction. This case highlights the need to consider food-related causes in patients with unexplained GI symptoms, even when the presentation is subtle or atypical.
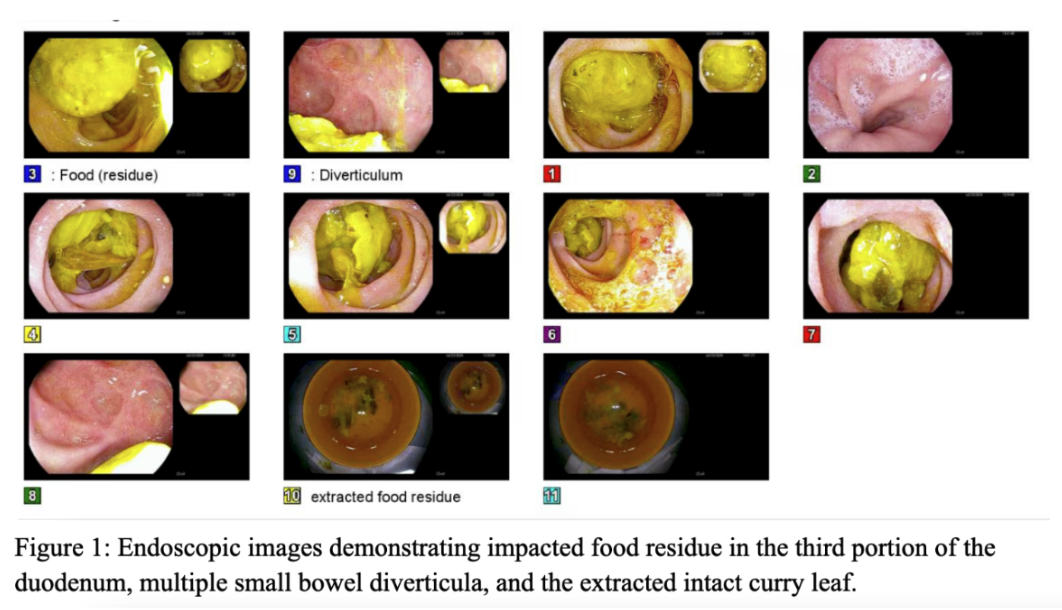
Figure: Figure 1: Endoscopic images demonstrating impacted food residue in the third portion of the duodenum, multiple small bowel diverticula and the extracted curry leaf