University of Cincinnati Medical Center Cincinnati, OH
Matthew Still, DO, Nathaniel Scarberry, MD, Susan Kais, MD, Christopher Mejia Juarez, MD, Anna Balog, MD University of Cincinnati Medical Center, Cincinnati, OH Introduction: Non-Hodgkin lymphomas (NHLs) involving the gastrointestinal (GI) tract can present with a range of nonspecific symptoms, as illustrated in this report of a 58-year-old male with well-controlled human immunodeficiency virus (HIV), who was diagnosed with diffuse large B-cell lymphoma (DLBCL). This case demonstrates the importance of including lymphoma in the differential diagnosis for individuals with HIV, regardless of CD4 count or antiretroviral therapy (ART) use.
Case Description/
Methods: The patient’s medical history included HIV, tobacco use, and obesity. He initially presented with non-bloody diarrhea, fever, and acute periumbilical pain that migrated to his right lower quadrant. Abdominal imaging showed thickening of the distal ileum, and laboratory studies showed a CD4 count of 877 cells/μL and a low viral load of 56 copies/mL. A colonoscopy performed six years prior was unremarkable. The differential diagnoses included inflammatory bowel disease, small bowel malignancy (given HIV, obesity, tobacco use), opportunistic infections, and ART-related complications. Bidirectional endoscopy was performed, and although esophagogastroduodenoscopy (EGD) was unremarkable, colonoscopy demonstrated ulcerated mucosa in the distal ileum. Biopsy revealed cytomegalovirus inclusions, and immunostains confirmed activated B-cell DLBCL, an aggressive lymphoma subtype. Positron emission tomography (PET) scan showed that the disease was limited to the distal ileum. The patient was referred to oncology and began chemotherapy. Discussion: Gastrointestinal lymphomas represent 10-15% of NHLs. However, primary GI lymphomas are relatively rare. DLBCL is the most common subtype of NHL, and the incidence of DLBCL is higher in patients with well-controlled HIV compared to immunocompetent individuals, with more than one-third of those diagnosed with HIV-related DLBCL presenting with CD4 counts > 200 cells/μL. The overall prognosis for patients with HIV-related DLBCL on ART is similar to that of HIV-negative patients, with two-year overall survival rates approximating 75%. Patients with HIV, even if well-controlled, are at a greater risk for lymphomas such as DLBCL. Including malignancy in the differential diagnosis in such patients can expedite diagnosis and care, as demonstrated by this case.
Artificial intelligence (AI) was used to assist in consolidating the content of this case report to align with submission criteria. The authors reviewed and edited all AI-generated material to ensure accuracy and integrity.
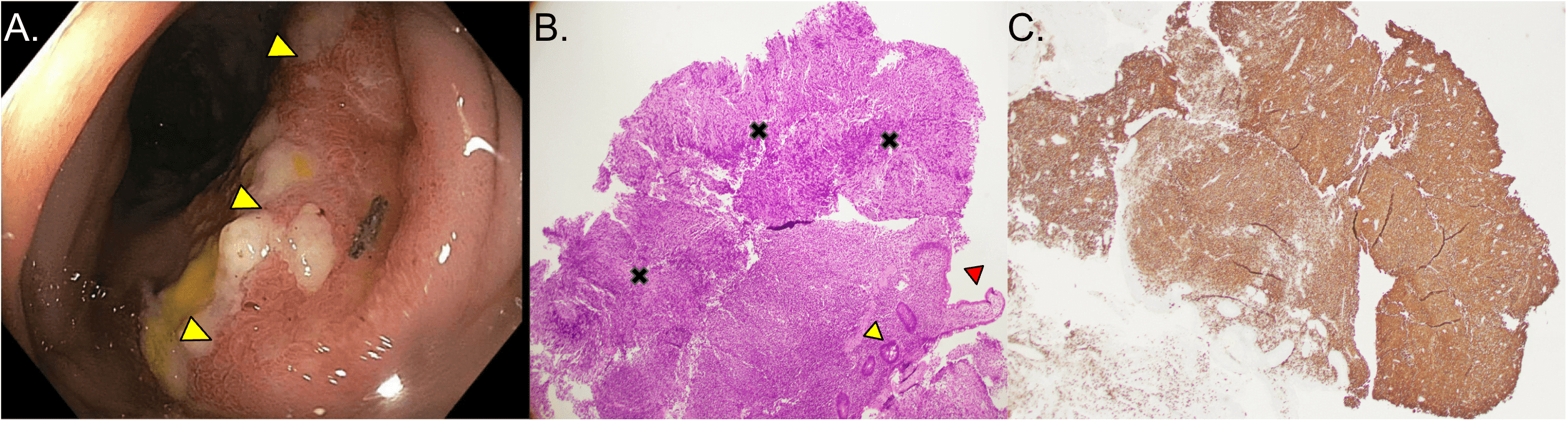
Figure: Figure 1. Gross and microscopic visualization of diffuse large B-cell lymphoma. A. Ulcerated and edematous lesion (yellow arrows) in the terminal ileum visualized by esophagogastroduodenoscopy. B. Histologic visualization of the terminal ileal lesion (40x): ileal crypt = yellow arrow, ileal epithelium = red arrow, tumor cells = black "x". C. CD20 immunohistochemical staining (brown) of the terminal ileal lesion, demonstrating the presence of B-cells.
Disclosures: Matthew Still indicated no relevant financial relationships. Nathaniel Scarberry indicated no relevant financial relationships. Susan Kais: Abbvie – Advisory Committee/Board Member, Marketing, Speakers Bureau. BMS – Advisory Committee/Board Member, Speakers Bureau. Jansen – Speakers Bureau. Christopher Mejia Juarez indicated no relevant financial relationships. Anna Balog indicated no relevant financial relationships.
Matthew Still, DO, Nathaniel Scarberry, MD, Susan Kais, MD, Christopher Mejia Juarez, MD, Anna Balog, MD. P4118 - Terminal Ileitis: An Unexpected Presentation of Diffuse Large B-Cell Lymphoma in Well-Controlled HIV, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.