University of Mississippi Medical Center Jackson, MS
Yassmin Hegazy, MD, Navdeep Kaur, MD, John Lam, MD, Satyapal Chahar, MD, Jeremy Morgan, MD, Shou-jiang Tang, MD University of Mississippi Medical Center, Jackson, MS Introduction: Duodenal-type follicular lymphoma (DFL) is a B-cell lymphoma that occurs in the duodenum and can be difficult to diagnose given its indolent course and subtle endoscopic findings. This is a case of DFL with negative surveillance scans that was initially diagnosed and treated as mucosa-associated lymphoid tissue (MALT) lymphoma prior to its recognition as a separate disease.
Case Description/
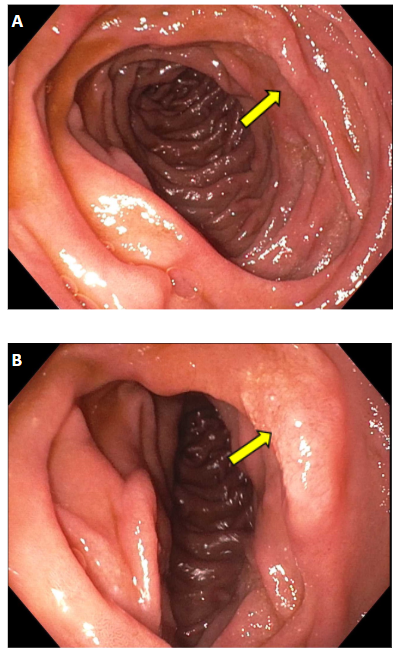
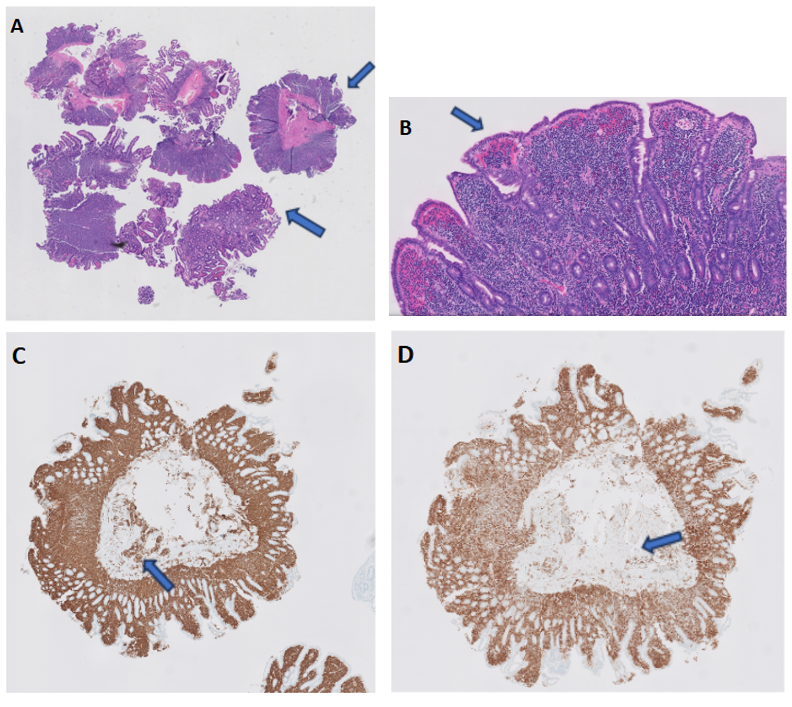
Methods: A 76 year-old female with a history of MALT lymphoma and Helicobacter pylori infection diagnosed and treated ten years prior to presentation with remission presents with continued abdominal pain. The patient presented for an outpatient endoscopic evaluation for disease surveillance. Recent Positron Emission Tomography (PET) scan did not show any abnormal uptake in the stomach or small intestine. The patient’s vitals, physical exam, and labs were unremarkable. EGD showed normal esophagus and stomach and patchy granular villi in the second portion of the duodenum that was biopsied with cold forceps (Figure 1A, 1B). Pathology revealed normal gastric mucosa and duodenal-type follicular lymphoma. The patient was recommended to continue her oral proton pump inhibitor and follow up with her hematologist for continued surveillance. The DFL was likely present on initial diagnosis ten years ago, however, was diagnosed as MALT lymphoma given the recent recognition of DFL as a separate disease entity. Discussion: DFL can be difficult to diagnose given its nuanced endoscopic features and need for biopsy. Originally classified as MALT, within the past ten years, DFL has become recognized as a separate diagnosis given its distinct histology and gene expression. While most patients are asymptomatic, abdominal pain and heartburn can occur with some patients having negative surveillance scans as seen in our case. Endoscopic findings of DFL include small, granular lesions between the duodenal villi most commonly in the second portion of the duodenum. Pathology shows lymphoid aggregates infiltrating the lamina propria (Figure 2A, 2B) and immunohistochemical staining demonstrates predominance of CD20-positive B-cells with many cells also expressing CD10 and BCL2, which are characteristic of follicular lymphoma as seen in our patient’s histology (Figure 2C, 2D). DFL is associated with a favorable prognosis given its indolent course and confinement to the submucosa and mucosa with radiation and chemoimmunotherapy used in patients with advanced stages. More studies are needed in order to better understand and identify DFL.
Figure: Figure 1A and Figure 1B: EGD showing patchy granular villi (yellow arrows) in the second portion of the duodenum.
Figure: Low power (Figure 2A) and high power (Figure 2B) histopathology slides with diffuse infiltration of the lamina propria by a monomorphic population of small lymphocytes (blue arrows). Histopathology slides showing CD20 (Figure 2C) and CD10 (Figure 2D) highlights in neoplastic B cells (blue arrows) in the lamina propria.
Disclosures: Yassmin Hegazy indicated no relevant financial relationships. Navdeep Kaur indicated no relevant financial relationships. John Lam indicated no relevant financial relationships. Satyapal Chahar indicated no relevant financial relationships. Jeremy Morgan indicated no relevant financial relationships. Shou-jiang Tang indicated no relevant financial relationships.
Yassmin Hegazy, MD, Navdeep Kaur, MD, John Lam, MD, Satyapal Chahar, MD, Jeremy Morgan, MD, Shou-jiang Tang, MD. P4108 - A Case of Duodenal-Type Follicular Lymphoma With Negative Surveillance Imaging, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.