Detroit Medical Center/Wayne State University Detroit, MI
Deema Almansour, DO, MS, Kenan Abou Chaer, MD, Majd Khadra, MD, Raya Abu Tawileh, MD, Aabid Mohiuddin, DO, Wael Dahhan, MD Detroit Medical Center/Wayne State University, Detroit, MI Introduction: Autoimmune hepatitis (AIH), primary biliary cholangitis (PBC) and primary sclerosing cholangitis (PSC) are the major autoimmune liver disorders. When clinical, serologic or histologic features of more than one disease coexist, the condition is termed an overlap syndrome. AIH-PBC overlap is the most frequently encountered, affecting approximately 8–9% of patients. Despite its clinical relevance, diagnostic criteria has low sensitivity and diagnosis often requires integration of labs, histology and treatment response. This case emphasizes the diagnostic value of liver biopsy in identifying AIH features not apparent on serologic testing and highlights the importance of early combined therapy to prevent disease progression.
Case Description/
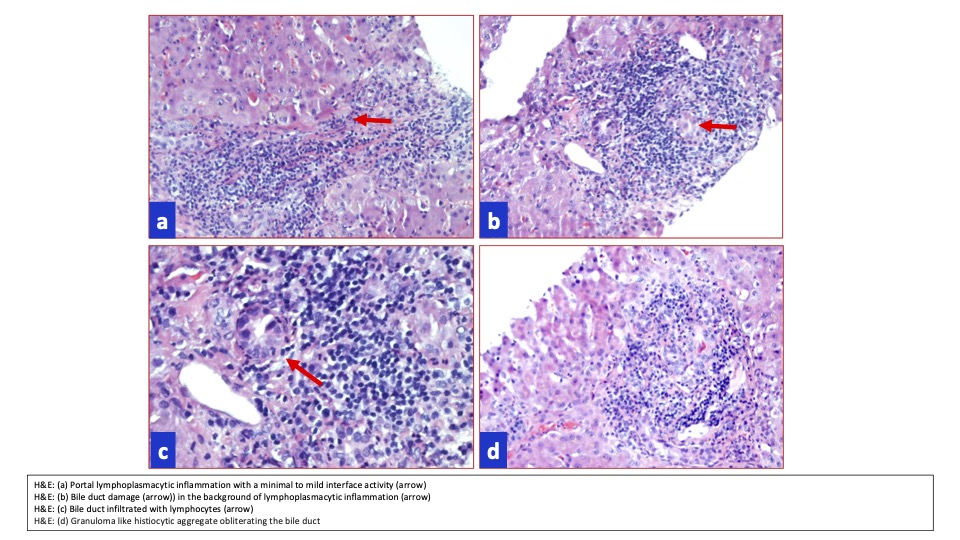
Methods: A 58-year-old African American woman with a medical history of hypertension and hyperlipidemia presented for complaints of fever, chills and malaise. Vitally, the patient was febrile and tachycardic. Physical exam was remarkable for scleral icterus, later developing encephalopathy. Labs showed a total bilirubin of 12.77 mg/dL, direct bilirubin of 6.88 mg/dL, ALT of 253 U/L, AST of 47 U/L and GGT of 73 U/L. AMA was 29.7 U, but SMA was unremarkable. ANA was weakly positive with a titer of 1:80. Intrahepatic and extrahepatic dilation were not seen on MRCP. Liver biopsy showed portal bile duct injury and florid duct lesions, consistent with PBC. Portal and lobular inflammation along with interface hepatitis also seen, compatible with AIH. These findings prompted the switch from pulse-dose methylprednisolone to prednisone and ursodiol, which led to the downtrend of bilirubin and transaminases and resolution of encephalopathy.
Discussion: AIH-PBC overlap syndrome presents a diagnostic challenge due to the lack of standardized criteria. Our patient had lab findings suggestive only of PBC, including positive AMA and elevated GGT, without AIH indicators. However, liver biopsy revealed interface hepatitis and portal inflammation, consistent with AIH features. Her significant improvement with combined ursodiol and immunosuppressive therapy confirmed the overlap diagnosis. This case highlights the importance of histologic evaluation in suspected overlap syndromes. Relying solely on serologic and biochemical markers may delay appropriate treatment. Early biopsy can uncover hidden disease components and guide optimal therapy to prevent progression and fibrosis.
Figure: AIH-PBC histology slides from liver biopsy
Disclosures: Deema Almansour indicated no relevant financial relationships. Kenan Abou Chaer indicated no relevant financial relationships. Majd Khadra indicated no relevant financial relationships. Raya Abu Tawileh indicated no relevant financial relationships. Aabid Mohiuddin indicated no relevant financial relationships. Wael Dahhan indicated no relevant financial relationships.
Deema Almansour, DO, MS, Kenan Abou Chaer, MD, Majd Khadra, MD, Raya Abu Tawileh, MD, Aabid Mohiuddin, DO, Wael Dahhan, MD. P4014 - A Diagnostic Challenge: Autoimmune Hepatitis–Primary Biliary Cholangitis Overlap Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.