University of Texas Rio Grande Valley Edinburg, TX
Kashif Ali, MD1, Asif Zamir, MD, FACG2 1University of Texas Rio Grande Valley, Edinburg, TX; 2DHR Health Gastroenterology, Edinburg, TX Introduction: Acute liver failure (ALF) is associated with high mortality and morbidity and is typically caused by viruses, drug-induced, or autoimmune conditions, often requiring liver transplantation(LT). Heat stroke leading to ALF is a rare etiology, and its spontaneous recovery without a LT is not well documented in the literature. Herein, We present a case of ALF in a young patient caused by heat stroke, managed successfully with conservative treatment.
Case Description/
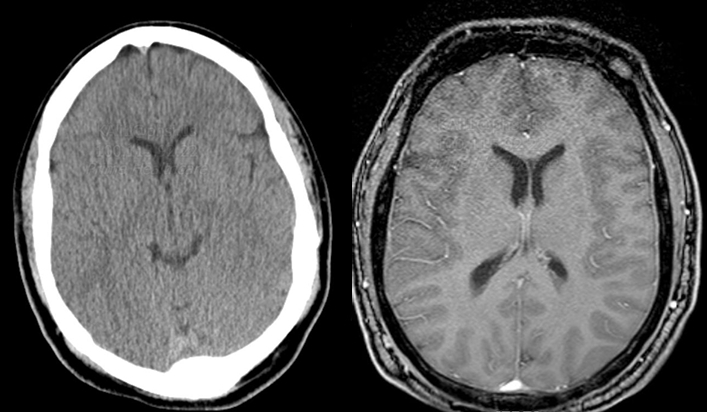
Methods: A 27-year-old male with no known comorbidities was brought to the Emergency Department (ED) in an unresponsive state. His maximum recorded temperature was 106°F, blood pressure was 70/30 mmHg, heart rate was 104 bpm, and respiratory rate was 23 breaths per minute. His Glasgow Coma Scale (GCS) score was 3, and he lacked cough, gag, and pupillary reflexes. Jaundice was noted on the exam. Initial management included intubation, conservative measures such as sedation, cooling pads, intravenous fluids, and vasopressor support. A computed tomography (CT) scan showed no intracranial bleeding. Initial laboratory results revealed an acetaminophen level of 0, salicylate level of 0, negative autoimmune workup, ALT of 8,096 U/L, AST of 10,376 U/L, INR > 9.1, fibrinogen < 54 mg/dL, and ammonia level of 142 µmol/L. An abdominal ultrasound was unremarkable. During his hospital stay, he had one episode of melena. An esophagogastroduodenoscopy showed no active bleeding. He received two units of fresh frozen plasma and one unit of cryoprecipitate. LT evaluation was recommended; however, transfer to an LT center was denied due to social factors. His renal function worsened (BUN 60, creatinine 10 mg/dL), prompting initiation of continuous renal replacement therapy. An MRI revealed occipital cortical edema consistent with posterior reversible encephalopathy syndrome. He gradually improved, with liver enzymes decreasing to ALT 250 U/L and AST 325 U/L, platelets rising to 325 × 10⁹/L, and INR improving to 1.2. In the following days, he regained reflexes, was extubated, began following commands, remained on room air, and was subsequently discharged to a rehabilitation unit. Discussion: Heat stroke is a life-threatening condition causing multiorgan failure. Management of ALF should prioritize resuscitation and stabilization. LT is recommended for patients unresponsive to initial treatment. In this case, young age and lack of comorbidities likely contributed to recovery without transplant, highlighting the critical role of early resuscitation.
Figure: No parenchymal hemorrhage and no midline shift on brain imaging.
Disclosures: Kashif Ali indicated no relevant financial relationships. Asif Zamir indicated no relevant financial relationships.
Kashif Ali, MD1, Asif Zamir, MD, FACG2. P4012 - Acute Liver Failure in a Young Adult Due to Exertional Heat Stroke: Recovery Following Supportive Care - A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.