Huzaif Taufiq, MD1, Mahnoor Tariq, MBBS2, Kavina Munshi, DO3, Ashley Gault, DO3, Haris Taufiq, MBBS4, Mohammed Shakhatreh, MD3 1Jefferson Torresdale Hospital, Willow Grove, PA; 2NA, Willow Grove, PA; 3Jefferson Torresdale Hospital, Philadelphia, PA; 4Ziauddin University, Karachi, Sindh, Pakistan Introduction: Primary biliary cirrhosis (PBC) and autoimmune hepatitis (AIH) are two main immune-mediated liver diseases. Some patients display characteristics of both diseases, so called overlap syndrome. This variant occurs in 3-7% of patients with autoimmune liver disease. It is rare, and its optimal treatment is uncertain. Patients with overlap syndrome typically present with both hepatic and cholestatic serum liver test abnormalities, as well as histological features of both AIH and PBC. We present a case of an 18-year-old man who developed AIH and PBC
Case Description/
Methods: Patient presented to the hospital with elevated liver enzymes and developed jaundice. Patient denies abdominal pain, nausea, vomiting, and weight loss. There was no family history of liver disease and no alcohol use. An outpatient workup revealed positive ANA and elevated IgG levels. Patient had tests done which were negative for Anti-smooth muscle, Urine drug screen, EBV, HSV, CMV, and Hepatitis A, B and C. However, anti-mitochondrial antibody was positive.
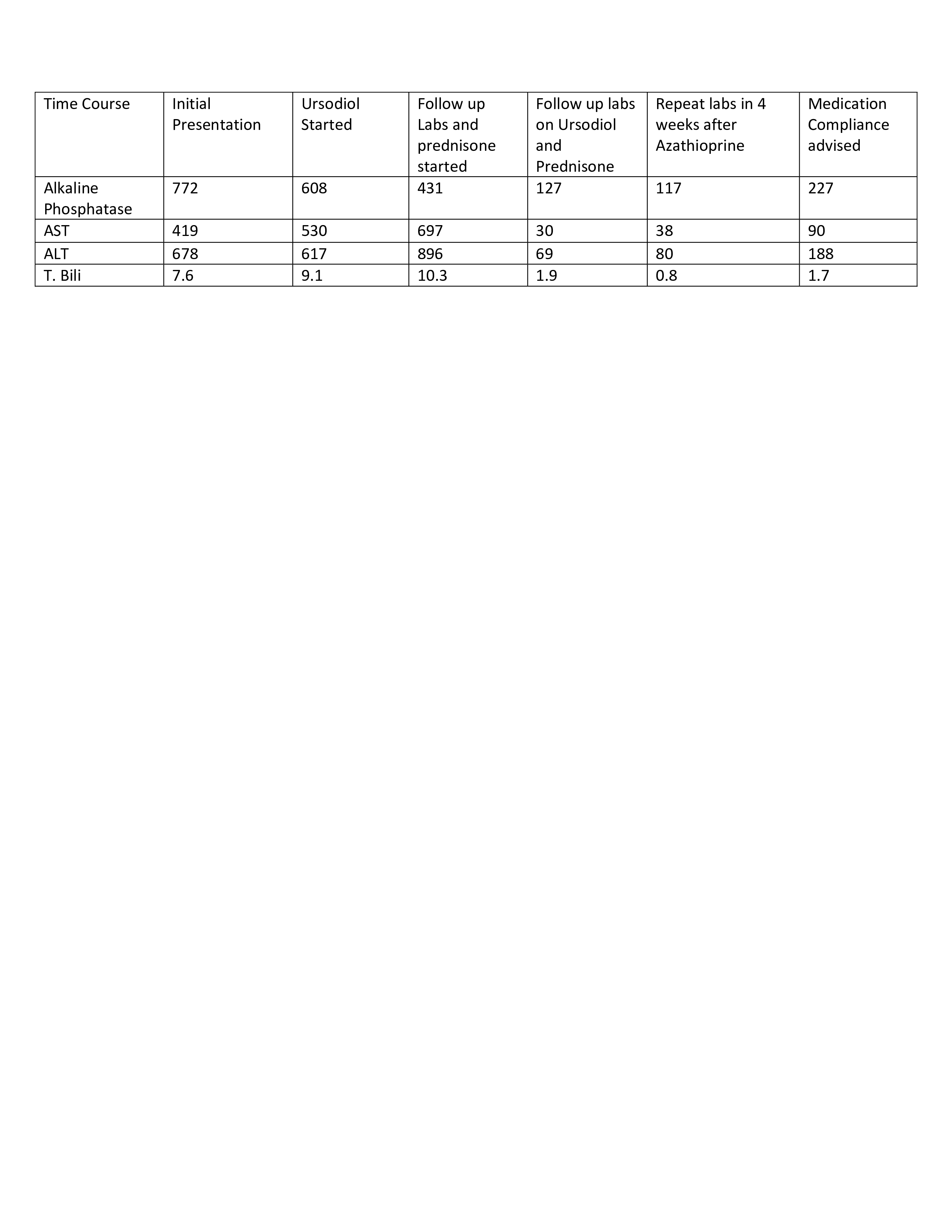
A liver biopsy was performed, and the patient was started on ursodiol for primary biliary cholangitis, with no improvement in his liver enzymes. Subsequently, Liver biopsies were re-reviewed by the pathologist and gastroenterologist with concern of autoimmune hepatitis and primary biliary cirrhosis with a picture of overlap syndrome. Patient was started on prednisone along with ursodiol.
Patient liver enzymes started to improve. Prednisone was decreased and patient was started on azathioprine. Patient was regularly scheduled for follow up with Gastroenterology. Patient admits being compliant with azathioprine and prednisone but not ursodiol. Medication compliance was advised, and patient is being followed closely with the gastroenterologist Discussion: AIH-PBC is the overlap syndromes and should always be kept in mind by clinicians while diagnosing. Early diagnosis and intervention of this condition are required for the better outcome of the patient. If left untreated, patients with overlap syndrome will have higher rates of portal hypertension, gastrointestinal bleeding, ascites, death, and need for liver transplant. Medical treatment of AIH-PBC is empiric and includes anticholestatic therapy of the cholestatic component and immunosuppressive therapy with corticosteroids and azathioprine of the hepatitis component of these disorders. If progressed to end stage disease, liver transplantation will be required
Figure: Patient's liver enzymes were closely monitored as various treatments were added
Disclosures: Huzaif Taufiq indicated no relevant financial relationships. Mahnoor Tariq indicated no relevant financial relationships. Kavina Munshi indicated no relevant financial relationships. Ashley Gault indicated no relevant financial relationships. Haris Taufiq indicated no relevant financial relationships. Mohammed Shakhatreh indicated no relevant financial relationships.
Huzaif Taufiq, MD1, Mahnoor Tariq, MBBS2, Kavina Munshi, DO3, Ashley Gault, DO3, Haris Taufiq, MBBS4, Mohammed Shakhatreh, MD3. P4008 - When 2 Autoimmune World Collides: A Rare Overlap Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.