University of Texas Health San Antonio San Antonio, TX
Emilio Fernandez, MD1, Grecia Dominguez Rivera, MD1, Eugenia Tsai, MD2, Lisa D. Pedicone, PhD2, Andres Gomez-Aldana, MD2, Carmen Landaverde, MD2, Jan Petrasek, MD, PhD2, Eric Lawitz, MD3, Fred Poordad, MD2, Fabian Rodas, MD2 1University of Texas Health San Antonio, San Antonio, TX; 2Texas Liver Institute, Austin, TX; 3Texas Liver Institute, San Antonio, TX Introduction: Mycobacterium avium complex (MAC), an environmental pathogen acquired via inhalation or ingestion, frequently causes disseminated disease in immunocompromised patients, notably those with AIDS. Hepatic involvement occurs in over 50% of disseminated cases, often manifesting as granulomatous liver disease. We present a case of a patient who developed transaminitis and new-onset ascites in the setting of granulomatous liver disease secondary to disseminated MAC.
Case Description/
Methods: A 27-year-old male with a past medical history of AIDS and disseminated MAC was directly admitted due to chronic diarrhea and MAC bacteremia. The patient was initially diagnosed with disseminated MAC in February 2024 and closely followed by ID with outpatient antibiotic management (rifabutin, ethambutol, and azithromycin). In late December 2024, the patient was admitted for esophageal candidiasis. Blood cultures at that time were positive for MAC with new resistances. The patient was admitted and began treatment with IV amikacin. During admission, the patient developed elevated liver-associated enzymes, AST 160 U/L, ALT 142 U/L, and ALP 518 U/L with new-onset ascites. A CT liver 4 phase was only significant for mild hepatomegaly. Paracentesis was performed with studies showing a serum-ascites albumin gradient of 1.3. An IR-guided transjugular liver biopsy was consistent with portal hypertension (portal gradient=22 mm Hg). Histology showed hepatic parenchyma with multiple non-necrotizing poorly formed granulomatous containing acid-fast bacilli, consistent with MAC. The patient was discharged on ethambutol, rifabutin, azithromycin, and IV amikacin. At a recent follow-up, the patient reports resolution of diarrhea, though he has still required 3 paracenteses in the 3 months following discharge. His liver-associated enzymes have since down trended and are now near or within normal limits: AST 19 U/L, ALT 16 U/L and ALP 179 U/L. Discussion: Hepatic granulomas are observed in 2% to 10% of all liver biopsy specimens and are a hallmark of disseminated Mycobacterium avium complex infection, particularly in immunocompromised patients. Non-cirrhotic portal hypertension, as seen in this case, is a rare complication of granulomatous liver disease. Clinically, patients may present with ascites and other sequelae of portal hypertension. Pathophysiology involves granulomatous inflammation compressing intrahepatic venous lumina, coupled with fibrosis from resolving granulomas, which leads to elevated portal pressures.
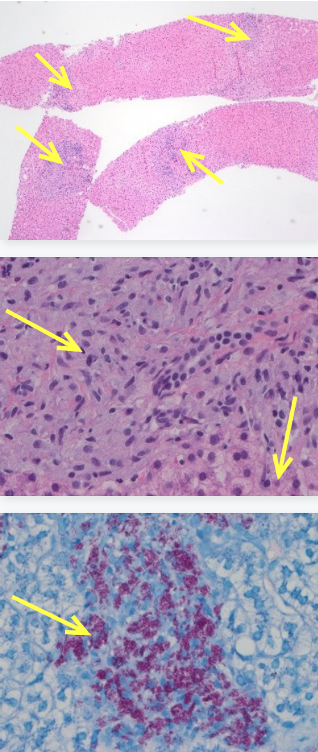
Figure: Fig 1. Low-power (40X mag) H&E with multiple non-necrotizing granulomata involving hepatic parenchyma. Fig 2. High-power (400X mag) H&E with non-necrotizing granuloma and also bile duct and hepatocytes in lower right. Fig 3. High-power (400X mag) Ziehl-Neelsen stain highlights abundant acid-fast bacilli.
Emilio Fernandez, MD1, Grecia Dominguez Rivera, MD1, Eugenia Tsai, MD2, Lisa D. Pedicone, PhD2, Andres Gomez-Aldana, MD2, Carmen Landaverde, MD2, Jan Petrasek, MD, PhD2, Eric Lawitz, MD3, Fred Poordad, MD2, Fabian Rodas, MD2. P3980 - Under Pressure: Granulomatous Liver Disease and Portal Hypertension in Disseminated MAC, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.