George Washington University Hospital Washington, DC
Vinay Rao, MD1, Melissa Kaltenbach, MD2, Edina Paal, MD2, Jessica PE. Davis, MD, MSCR2, Atoosa Rabiee, MD, FACG2 1George Washington University Hospital, Washington, DC; 2Washington DC VA Medical Center, Washington, DC Introduction: The prevalence of hepatitis D virus (HDV) and hepatitis E virus (HEV) remains low in the US. Concomitant infection with HDV and HEV is even rarer with only a few cases reported. We present an unusual case of a patient exposed to four hepatitis infections: chronic active hepatitis B virus (HBV) and prior hepatitis C virus (HCV) evaluated for acute liver injury found to be positive for HDV and HEV.
Case Description/
Methods: 71-year-old male with a history of chronic HBV compensated cirrhosis nonadherent to tenofovir initially hospitalized for hip fracture developed elevated liver function tests (LFTs) in a hepatocellular injury pattern. AST and ALT were initially 2-3 times the upper limit of normal (ULN) but rose to a peak of 15-20 times the ULN. Alkaline phosphatase was mildly elevated. Total bilirubin and INR were normal. Initial workup noted nonreactive hepatitis A virus (HAV) total and IgM, reactive HBsAg and HBcAb total with viral load (VL) of 360,000, and reactive HCV Ab with undetectable viral load. One week after restarting tenofovir a repeat VL was 20,000. Due to worsening enzyme elevation, percutaneous liver biopsy was performed and revealed severe portal and lobular hepatitis with focal ground-glass hepatocytes. HBsAg staining was positive. Given concerns for a secondary viral process additional labs were obtained notable for detectable HDV RNA and reactive HEV IgM with nonreactive IgG. LFTs ultimately improved and the patient was discharged with a plan to perform confirmatory quantitative HDV and HEV VLs and discuss HDV treatment, however the patient was lost to follow up. Discussion: Our patient’s case was notable for HDV superinfection on chronic HBV and possible acute HEV infection. The acute rise in LFTs was likely due to HDV although true VL remains unknown due to loss to follow up. HDV is important to exclude given increased risk of fibrosis progression and hepatocellular carcinoma with concurrent HBV. Treatment considerations include initiating pegylated interferon-alfa for HDV and tenofovir for HBV. HEV is important to consider in patients with immune suppression, solid organ transplantation, and chronic liver disease. While HEV IgM was reactive, assay accuracy for HEV antibodies is highly variable and can report false positives due to cross-reactivity with other viruses. A VL would be needed for confirmation of acute infection. This unique case highlights the importance of a comprehensive workup for acute liver injury including consideration of less common viral hepatitides.
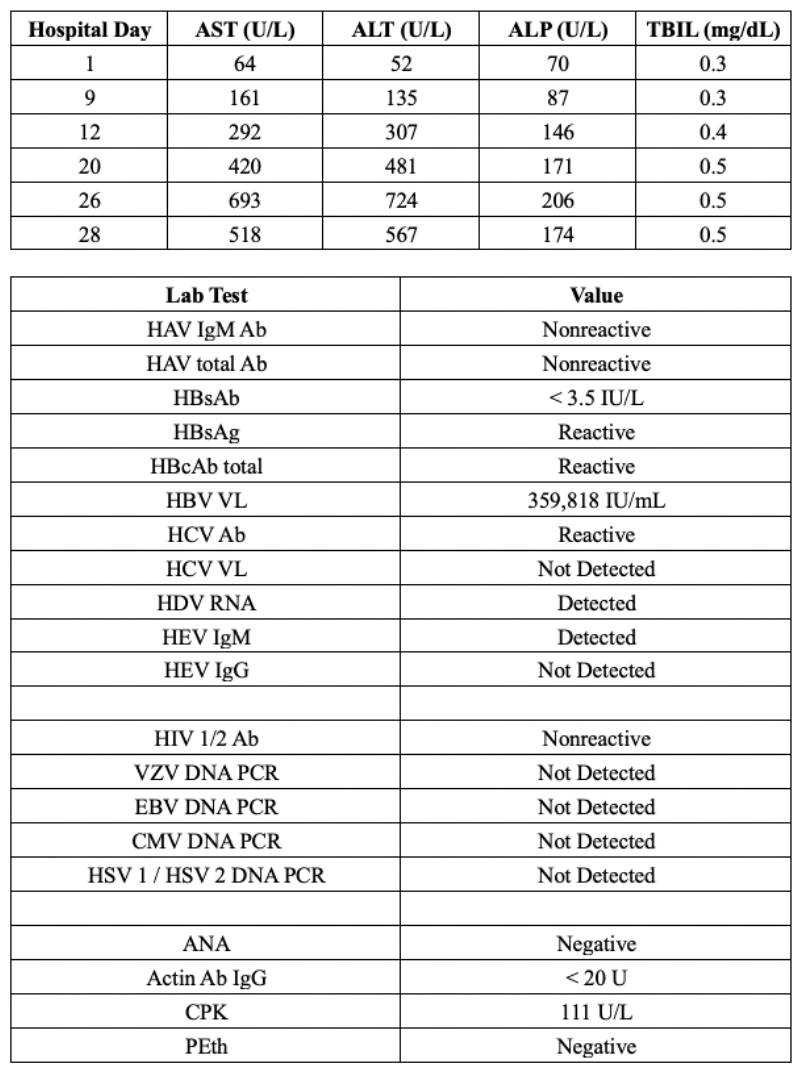
Figure: Table 1: Trend in liver function tests (LFTs) during hospitalization and summary of serologic workup.
(AST: aspartate aminotransferase; ALT: alanine aminotransferase; ALP: alkaline phosphatase; TBIL: total bilirubin; HAV: hepatitis A virus; Ab: antibody; HBV: hepatitis B virus; VL: viral load; HCV: hepatitis C virus; HDV: hepatitis D virus; HEV: hepatitis E virus; HIV: human immunodeficiency virus; VZV: varicella zoster virus; EBV: Epstein-Barr virus; CMV: cytomegalovirus; HSV: herpes simplex virus; ANA: antinuclear antibody; CPK: creatine phosphokinase; PEth: phosphatidylethanol).
Figure: Figure 1: Percutaneous liver biopsy sections demonstrating severe portal and lobular hepatitis composed of lymphocytes and plasma cells with focal ground-glass hepatocytes at 10X (panel A) and 20X (panel B) magnification and immunohistochemical staining positive for hepatitis B surface Ag (HBsAg) at 20X magnification (panel C).
Disclosures: Vinay Rao indicated no relevant financial relationships. Melissa Kaltenbach indicated no relevant financial relationships. Edina Paal indicated no relevant financial relationships. Jessica Davis indicated no relevant financial relationships. Atoosa Rabiee indicated no relevant financial relationships.
Vinay Rao, MD1, Melissa Kaltenbach, MD2, Edina Paal, MD2, Jessica PE. Davis, MD, MSCR2, Atoosa Rabiee, MD, FACG2. P3974 - The ABCDE's of Viral Hepatitis: A Case Presentation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.