Jenny Joseph, MBBS1, Mohammed Al-Aquily, MD1, Zablon Sewalem, MD, MSc1, Rammy Bashir, MD, MSc1, Triston Berger, MD2, Joseph Lim, MD3 1Norwalk Hospital/Yale University, Norwalk, CT; 2Norwalk Hospital, Norwalk, CT; 3Yale New Haven Hospital, New Haven, CT Introduction: Primary Biliary Cholangitis (PBC) is an autoimmune disease that results from inflammation and progressive destruction of biliary ducts. Anti-mitochondrial antibody (AMA) is a highly specific and sensitive marker of PBC; however, it is absent in 5% of cases. AMA-negative PBC remains a challenging diagnosis to establish. It presents with a cholestatic pattern of liver enzymes and can be difficult to distinguish from other common causes of liver disease, such as fatty liver. We present a case of AMA-negative PBC which was attributed to fatty liver disease for many years prior to presentation.
Case Description/
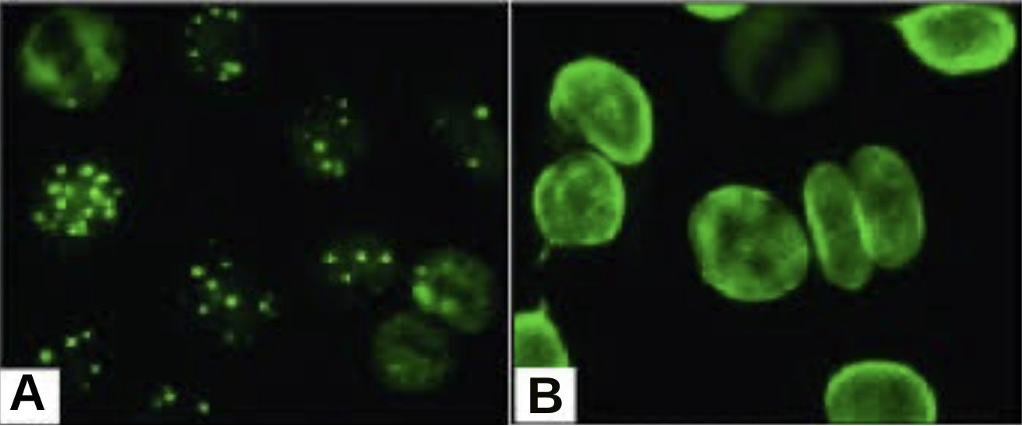
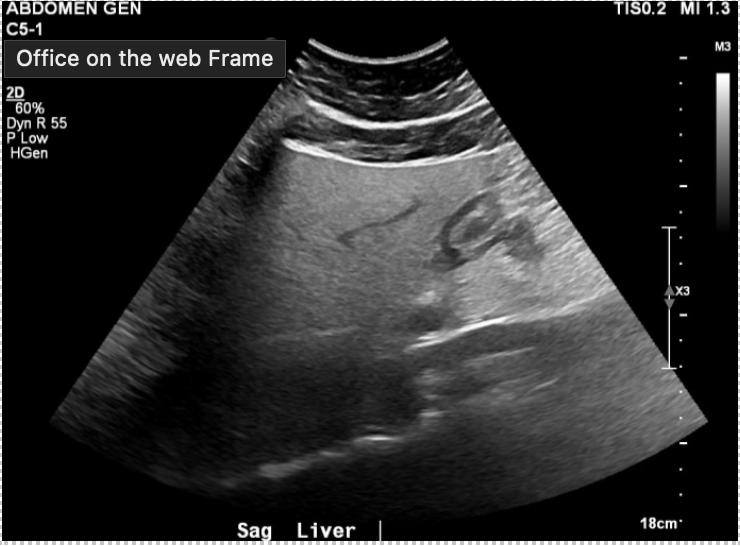
Methods: 55-year-old female with obesity, hypothyroidism, and recently treated endometrial and ovarian cancer was referred to hepatology for evaluation of chronically elevated alkaline phosphatase (ALP). She was noted to have persistently elevated ALP for several years, attributed to obesity and hepatic steatosis described in imaging (Fig 1). Prior to evaluation by hepatology, she never had a formal serologic workup. ALP fractionation confirmed hepatic origin. Hepatitis panel was negative. She was AMA negative but had positive Antinuclear antibodies (ANA) with nuclear dots pattern. This prompted further testing including anti-gp210 and anti-sp100 antibodies, the latter of which was positive. Non-invasive fibrosis assessment (ultrasound with elastography, Fibrosure) was negative. She was diagnosed with AMA-negative PBC and started on ursodiol with regular hepatology follow-up. Discussion: Although elevated ALP is common in the setting of obesity and hepatic steatosis, it is important not to anchor on this diagnosis and to evaluate for other underlying causes, as a missed diagnosis can lead to permanent hepatic injury. AMA is the hallmark of PBC but is negative in 5% of cases. It is important to be able to recognize other markers with high specificity for PBC, which can help diagnose AMA negative cases. Although ANA with nuclear dots/rim-like pattern (Fig 2 A, B), anti-sp100, and anti-gp210 have low sensitivities, their specificities are greater than 98%. These tests help in early recognition of AMA negative PBC which then lead to appropriate treatment that can slow disease activity and progressive hepatic injury.
Figure: Fig 1 Ultrasound of the abdomen showing hepatic steatosis
Figure: Fig 2 (A) ANA with nuclear dot pattern (B) ANA with rim-like pattern
Disclosures: Jenny Joseph indicated no relevant financial relationships. Mohammed Al-Aquily indicated no relevant financial relationships. Zablon Sewalem indicated no relevant financial relationships. Rammy Bashir indicated no relevant financial relationships. Triston Berger indicated no relevant financial relationships. Joseph Lim indicated no relevant financial relationships.
Jenny Joseph, MBBS1, Mohammed Al-Aquily, MD1, Zablon Sewalem, MD, MSc1, Rammy Bashir, MD, MSc1, Triston Berger, MD2, Joseph Lim, MD3. P3969 - Beyond the Fatty Liver: A Challenging Diagnosis of Antimitochondrial Antibody-Negative Primary Biliary Cirrhosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.