Judith Njoroge, DO1, Hakizimana Niyoyita Adolphe, MD, Mmed2, Chioma Owo, MD3, Jean de Dieu Dushimimana, MD4, Joseph Musabyimana, MD, MPH, Mmed5, Sabine Nyiraneza, MD, Mmed5, Marie Solange Mukanumviye, MD5 1Des Moines University, Kankakee, IL; 2University of Rwanda, Kigali CIty, Kigali, Rwanda; 3University of Texas Health San Antonio, San Antonio, TX; 4University of Rwanda, Kigali City, Kigali, Rwanda; 5University Teaching Hospital of Kigali (CHUK), Kigali City, Kigali, Rwanda Introduction: Felty syndrome (FS), an autoimmune disorder that is a subset of seropositive rheumatoid arthritis (RA), is defined by severe RA, idiopathic neutropenia, and splenomegaly. Its estimated prevalence is 1-3% in the US, and likely lower in Africa. Diagnosis requires chronic idiopathic neutropenia and seropositive RA. Liver involvement is rare but may present as Non-Cirrhotic Portal Hypertension (NCPH), a potentially morbid complication.
Case Description/
Methods: A 63-year-old woman with no prior autoimmune diagnosis presented to the University Teaching Hospital of Kigali (CHUK) in April 2025 with early satiety, bloating, vomiting, and a chronic left foot wound. She also had chest discomfort, dry cough, night sweats, weakness, and 30 kg unintentional weight loss. Exam showed oral thrush, bilateral joint deformities, a left dorsal foot wound, and stage III splenomegaly. Labs showed severe neutropenia, anemia, mildly elevated ALP, normal transaminases and elevated anti-CCP, ESR/CRP, and rheumatoid factor. Infectious screening was negative. Bone marrow and foot biopsies ruled out dysplasia or malignancy. Chest CT showed pulmonary fibrosis. Abdominal CT showed hepatosplenomegaly, benign hepatic cysts, portal hypertension without cirrhosis or thrombosis. EGD showed antral gastritis, no varices, ulcers, or bleeding; colonoscopy was unremarkable. She was stabilized and started on empiric antibiotics. On day 5, after positive rheumatologic workup, she was started on oral prednisone, methotrexate, folic acid, and IV dexamethasone. By day 8, neutropenia had mildly improved and she was discharged. At 6-week follow-up, she had remained on prednisolone but stopped methotrexate and folic acid. Neutropenia had resolved, splenic size decreased by 0.6cm, her foot wound had healed, and she had resumed light daily activities. She did not follow up with rheumatology due to limited local access. Discussion: This rare case of FS-associated NCPH in Rwanda highlights the importance of considering systemic autoimmune etiologies in patients presenting with leukopenia and portal hypertension. Though liver biopsy wasn't performed due to limited resources, diagnostic workup supported a diagnosis of FS-associated NCPH. Resolution of neutropenia and clinical improvement following initiation of immunosuppressive therapy further support the diagnosis. Increased awareness of this presentation of NCPH is crucial for timely diagnosis and integrated management, especially in low-resource areas where delayed diagnosis may worsen outcomes.
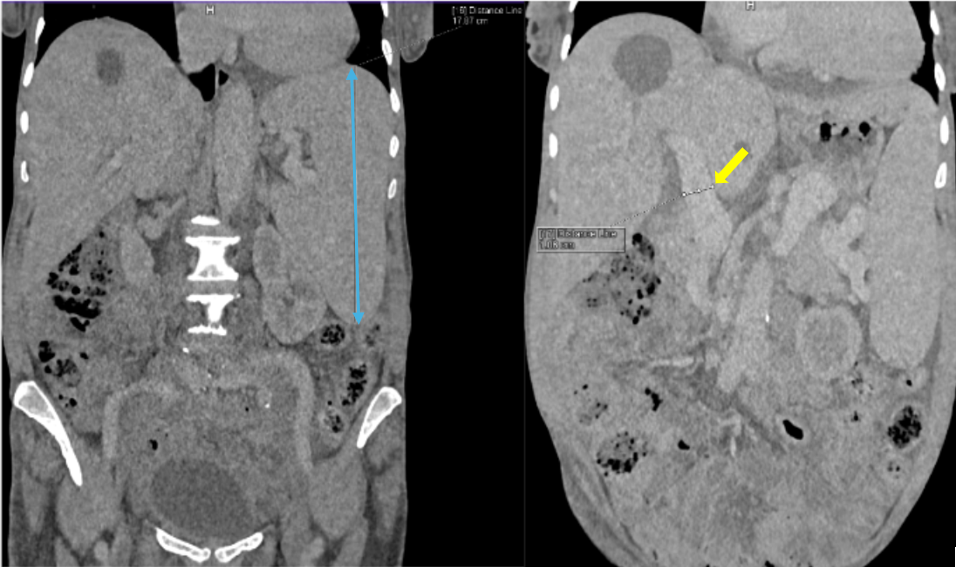
Figure: Figure 1: Contrast-enhanced abdominal CT images in the coronal plane illustrating splenomegaly and portal hypertension in a patient with Felty Syndrome. The left image shows splenomegaly (blue arrow) with a cranial-caudal splenic diameter of 17.87cm. The right image shows a dilated portal vein (yellow arrow) with a diameter measuring 1.86 cm. No radiographic evidence of cirrhosis or portal vein thrombosis is visualized. These findings are consistent with non-cirrhotic portal hypertension.
Figure: Figure 2: Clinical image showing bilateral joint deformities classically seen in long-standing rheumatoid arthritis. These deformities include ulnar deviation, metacarpophalangeal joint swelling, subtle atrophic changes of the intrinsic hand muscles, and swan neck deformity on the left hand. These findings, in addition to idiopathic neutropenia and splenomegaly, support the diagnosis of Felty syndrome.
Disclosures: Judith Njoroge indicated no relevant financial relationships. Hakizimana Niyoyita Adolphe indicated no relevant financial relationships. Chioma Owo indicated no relevant financial relationships. Jean de Dieu Dushimimana indicated no relevant financial relationships. Joseph Musabyimana indicated no relevant financial relationships. Sabine Nyiraneza indicated no relevant financial relationships. Marie Solange Mukanumviye indicated no relevant financial relationships.
Judith Njoroge, DO1, Hakizimana Niyoyita Adolphe, MD, Mmed2, Chioma Owo, MD3, Jean de Dieu Dushimimana, MD4, Joseph Musabyimana, MD, MPH, Mmed5, Sabine Nyiraneza, MD, Mmed5, Marie Solange Mukanumviye, MD5. P3931 - A Rare Case of Felty Syndrome-Associated Non-Cirrhotic Portal Hypertension in Sub-Saharan Africa, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")