Hayes Walker, MD, Madeline Wurst, MD, Samantha Whitwell, MD UTHSC, Memphis, TN Introduction: Desmoplastic small round cell tumor is a rare and highly aggressive malignancy, primarily affecting male adolescents and young adults. DSRCT typically arises from the serosal surfaces of the abdominal and pelvic cavities, frequently manifesting as multiple large masses with significant peritoneal involvement. Current management of DSRCT involves a multimodal approach including systemic chemotherapy, hyperthermic intraperitoneal chemotherapy, radiation, and surgical resection. Here we present a case of DSRCT presenting with biliary obstruction.
Case Description/
Methods: A 25-year-old female presented with two-weeks of scleral icterus, generalized pruritis, darkening of urine, pale stools, and back pain. She described a sensation of abdominal distension and “fullness” since childbirth eight months prior. A transvaginal ultrasound revealed fibroids and an ovarian cyst. Laboratory studies revealed elevated ALP, AST, ALT and total/direct bilirubin. CT scans revealed a heterogenous, hypoenhancing mass in the medial aspect of the medial hepatic lobe and associated intrahepatic biliary dilation. MRCP revealed a heterogeneous mass at the porta hepatis and a large heterogeneous mass within the abdominal mesentery, both with significant internal hypercellularity. ERCP with sphincterotomy was performed, along with pancreatic and common bile duct stent placements. Biopsies of the masses were sent to Mayo Clinic for analysis. Molecular cytogenetics helped to confirm her diagnosis of T4a,N0,M0 stage 3b desmoplastic small round cell carcinoma. The patient completed 6 cycles of VAC-IE (doxorubicin/vincristine/cyclophosphamide, iphosphomide/etoposide) alternating chemotherapy with minimal response. Doxorubicin was discontinued in the perioperative setting due to concern for cardiomyopathy. She underwent surgical resection of mesenteric/intra-abdominal mass, right partial liver resection, cholecystectomy, liver ablation, right colectomy, and ileocolic anastomosis. She is now awaiting clinical trial evaluation. Discussion: DSRCT is rare (0.3 cases/million) with a 4:1 male to female ratio. Prognosis is poor with a survival rate estimated at 33%. Definitive diagnosis of DSRCT relies on the identification of the EWSR1-WT1 gene fusion. This pathognomonic genetic mutation has been found to lead to the transcription of multiple targets involved in cellular proliferation, angiogenesis, and invasion. This case highlights a potential complication of DSRCT due to mass effect that can be alleviated with ERCP.
Figure: Sagittal CT image showing a heterogeneous, hypoenhancing mass in the medial aspect of the medial lobe of the liver with foci of spiculated calcification measuring approximately 11.9cm x 15.4cm by 18.0cm. Also noted is associated intrahepatic biliary dilatation.
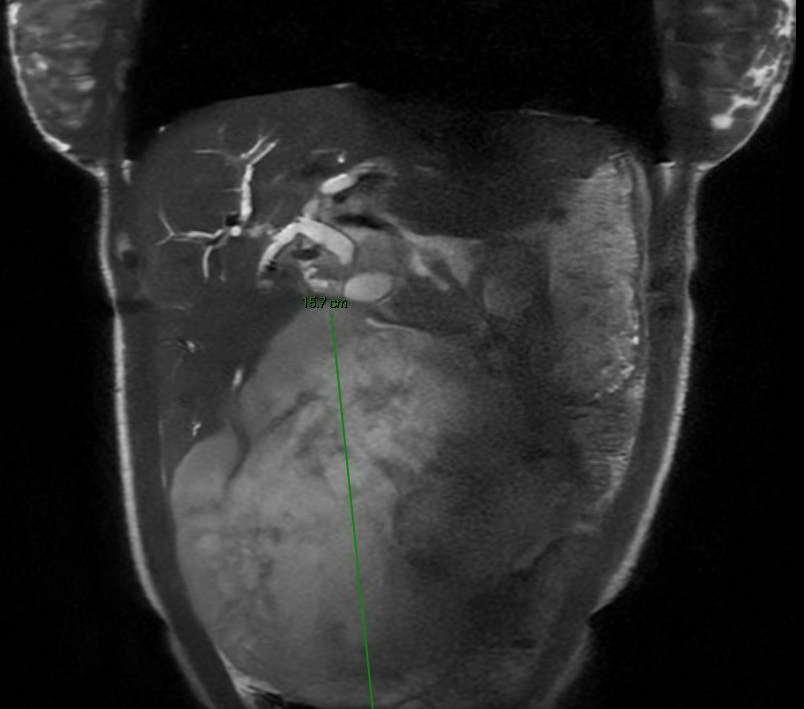
Figure: Coronal MR image showing a large heterogeneous mass within the abdominal mesentery with internal calcifications measuring up to 15.7cm x 15.2cm x 12.9cm in total extent.
Disclosures: Hayes Walker indicated no relevant financial relationships. Madeline Wurst indicated no relevant financial relationships. Samantha Whitwell indicated no relevant financial relationships.
Hayes Walker, MD, Madeline Wurst, MD, Samantha Whitwell, MD. P3923 - Desmoplastic Small Round Cell Tumor Presenting With Biliary Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.