Angela Torijano, MD1, Ronald Blanco Montecino, MD2, Ardijan Cobaj, MD1, Wendy Garzon, MD1, Suresh Nayudu, MD, FACG1 1St. Barnabas Hospital, Bronx, NY; 2St. Barnabas Hospital, New York, NY Introduction: Weil’s disease, a severe form of leptospirosis, is a rare but potentially life-threatening zoonotic infection caused by Leptospira species. It accounts for 5–10% of leptospirosis cases and is marked by multiorgan involvement, most notably acute kidney injury, hepatic dysfunction, and hemorrhagic manifestations. We present a rare case in a previously healthy 60-year-old male, highlighting diagnostic challenges and rapid clinical progression.
Case Description/
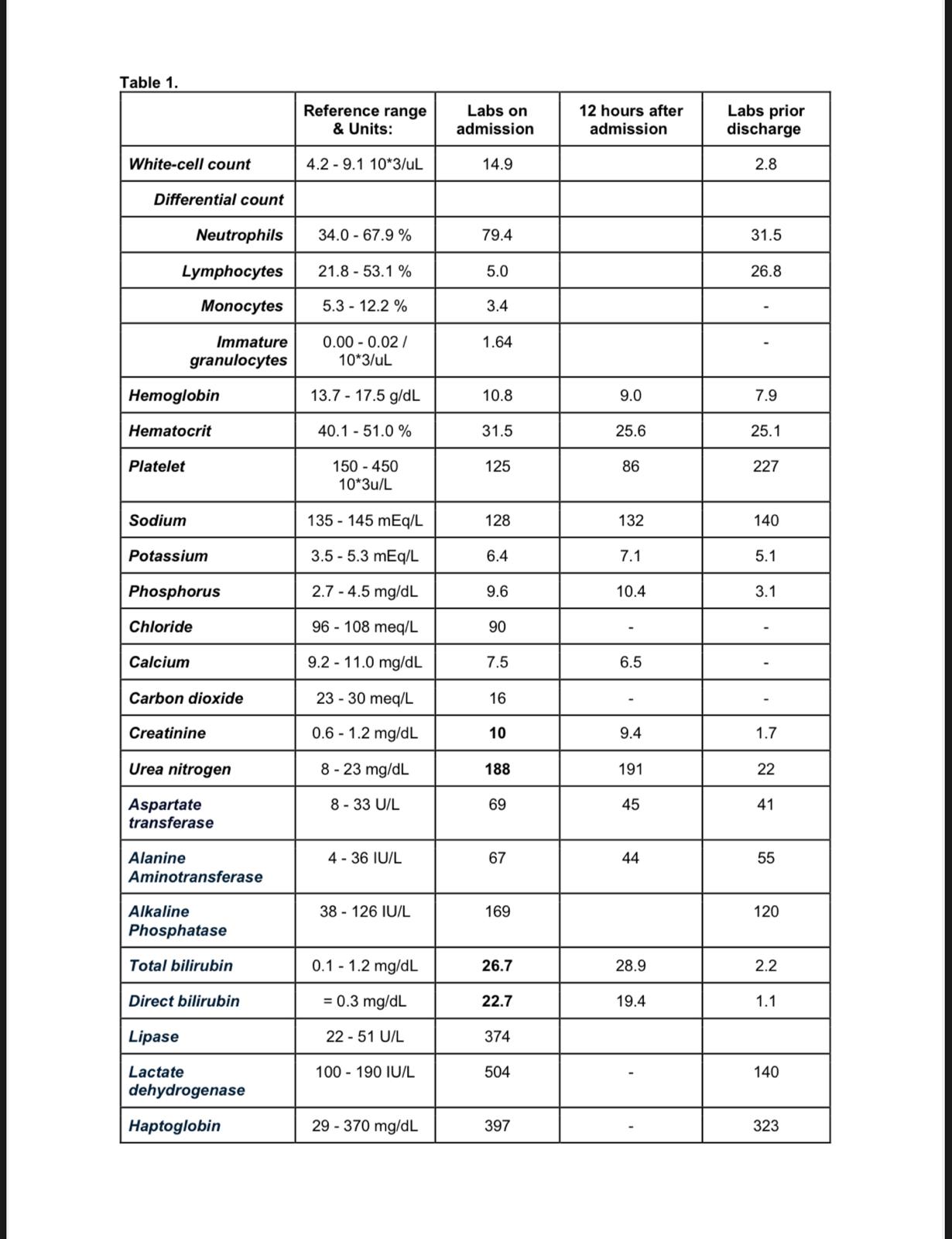
Methods: A 60-year-old male Albanian immigrant with no significant medical history presented to the emergency room with two weeks of progressive generalized malaise and night sweats. He denied fever, gastrointestinal symptoms, recent travel, or sick contacts. Initial evaluation revealed scleral icterus without any organomegaly. Labs showed severe acute kidney injury, with hyperkalemia, elevated liver enzymes, marked hyperbilirubinemia, and high alkaline phosphatase, suggesting renal and hepatocellular injury with cholestasis (Table 1). Also noted anemia with elevated LDH, low haptoglobin indicating hemolysis. Empiric antibiotics were initiated due to concerns for sepsis in the setting of leukocytosis, tachycardia, and hypotension. He was admitted to medical intensive care for further management and started on hemodialysis. Imaging (CT abdomen and pelvis) revealed a dilated bile duct, but MRCP ruled out obstruction and showed signs of portal hypertension.
Autoimmune hepatitis was considered due to positive antimitochondrial (AMA) and anti-smooth muscle (ASMA) antibodies, though Antinuclear antibodies were negative. However, his rapid clinical and biochemical improvement without corticosteroids argued against autoimmunity. Serologies were positive for Leptospira IgM and EBV PCR. Based on serologic evidence and clinical course, a diagnosis of Weil’s syndrome was made. The patient gradually improved with supportive management and was weaned off hemodialysis after two sessions. Discussion: Recognizing Weil’s disease is challenging as it can mimic several infectious and autoimmune diseases. Early recognition and treatment are crucial in managing these patients to prevent adverse outcomes. This case highlights the need to consider leptospirosis in patients with jaundice and renal failure, even in non-endemic regions.
Figure: Table 1.
Disclosures: Angela Torijano indicated no relevant financial relationships. Ronald Blanco Montecino indicated no relevant financial relationships. Ardijan Cobaj indicated no relevant financial relationships. Wendy Garzon indicated no relevant financial relationships. Suresh Nayudu indicated no relevant financial relationships.
Angela Torijano, MD1, Ronald Blanco Montecino, MD2, Ardijan Cobaj, MD1, Wendy Garzon, MD1, Suresh Nayudu, MD, FACG1. P3917 - Weil’s Disease Masquerading as Autoimmune Hepatitis: A Case of Severe Leptospirosis With Multiorgan Failure, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")